December 31st, 2013 §
I’ll be heading out soon to the hospital for two procedures. The first, a liver biopsy, will take samples of the small metastases to my liver for testing to get information about the cancer to help guide us in choosing targeted treatments. Features of cancer like hormone receptor status (ER, PR) and HER2 status can change over time and be varied in metastases in different parts of your body. It is important to repeat biopsies as time goes on to make sure you are still using the best drugs to treat your cancer.
The second procedure today is the implantation of a PleurX catheter. This will allow fluid to be removed from the lining of my left lung which has cancer in it. The fluid keeps accumulating so until we can get that reduced I will have to use this drain system at home to remove fluid daily. Keeping that level down will allow me to breathe well. This is a quite a process and I didn’t realize all that was involved. I’ll explain more about this in another post. This link shows how it works for anyone interested.
The main info I want to briefly share is that we now know more about where the excruciating pain I’ve been having is coming from. The PET showed that the cancer in my T12 vertebrae has grown and is encroaching on the space in my spinal canal. I also have an active spot of cancer that’s intense in my left hip. The spine, however, is where we are focusing the attention.
For now, we need to do more tests while I am in the hospital, but the immediate goal is to get radiation to my back and, if needed, to my pelvis. There is a lot to do to get all of that set but we are aiming to get radiation started by the end of the week. I do not know yet anything about what the protocol would be in terms of how many sessions but I do know that it will bring a lot of relief of pain once I can have that done. Until then it’s all about pain management.
I will also meet with a palliative care team while in the hospital to get the best assistance with the pain since it will be a while until I get relief at the source. Palliative care doctors are experts in pain management during all phases of cancer treatment, not just end of life. Palliative care teams help with side effects from the cancer and the treatments and are wonderful resources.
That’s all I have time to share for now but it looks like I still have a bit longer to wait for relief. Obviously this wasn’t news I wanted and I’m still adjusting to it. Once again, this latest development shows it doesn’t matter how you look on the outside; you can “look good” and still have cancer treatments that are not working, cancer that is progressing. This is an important message to repeat.
Right now we are still gathering information to decide whether I will participate in the clinical trial I was set to begin this week.
I hope you all have a safe New Year’s Eve and I’ll try to report back as soon as I can. Thank you for all of the support. It seems like a good time to once again share the link to my research fund donation page at Sloan Kettering in case anyone has those last minute end of year contributions to make!
December 29th, 2013 §
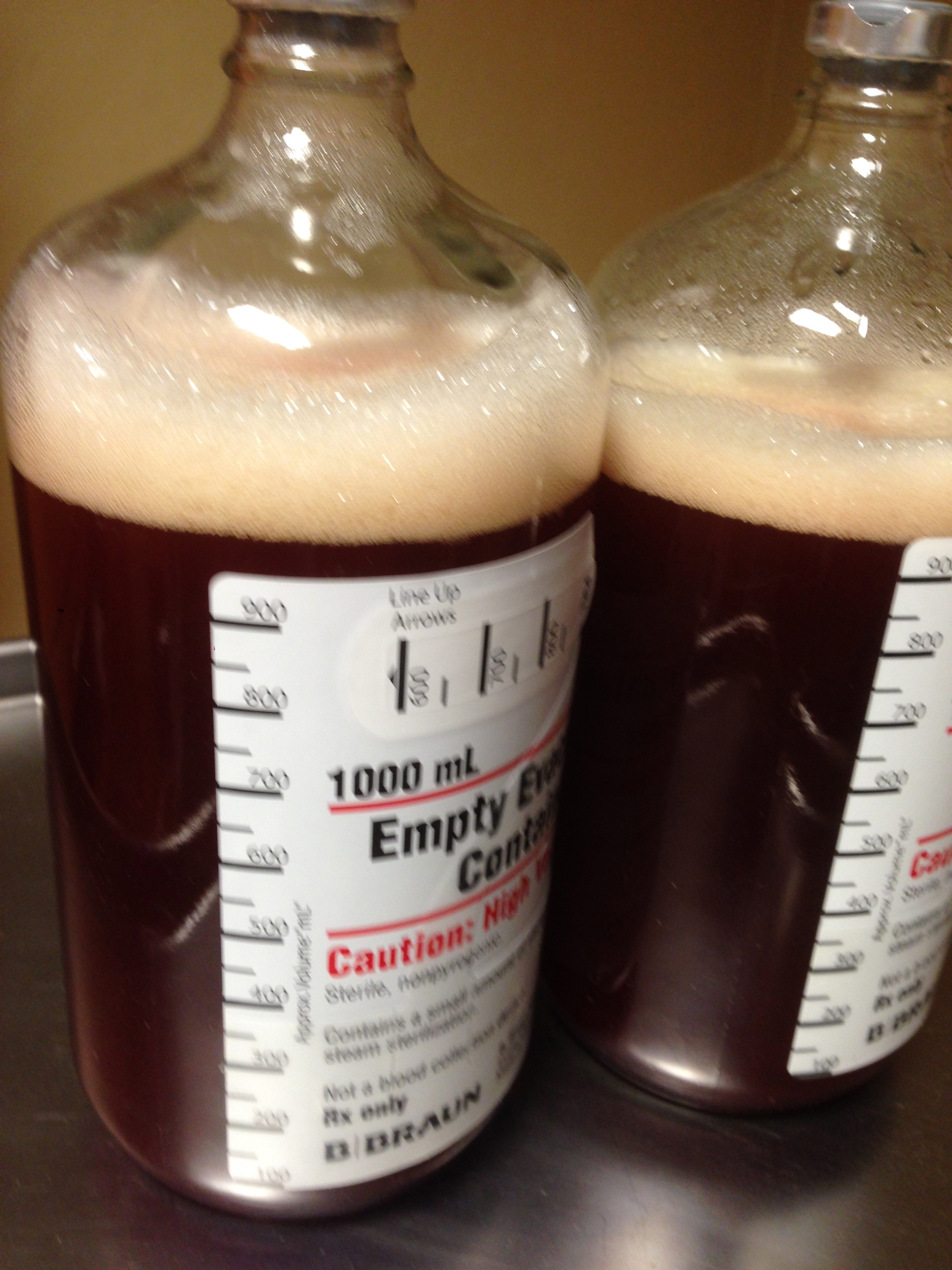
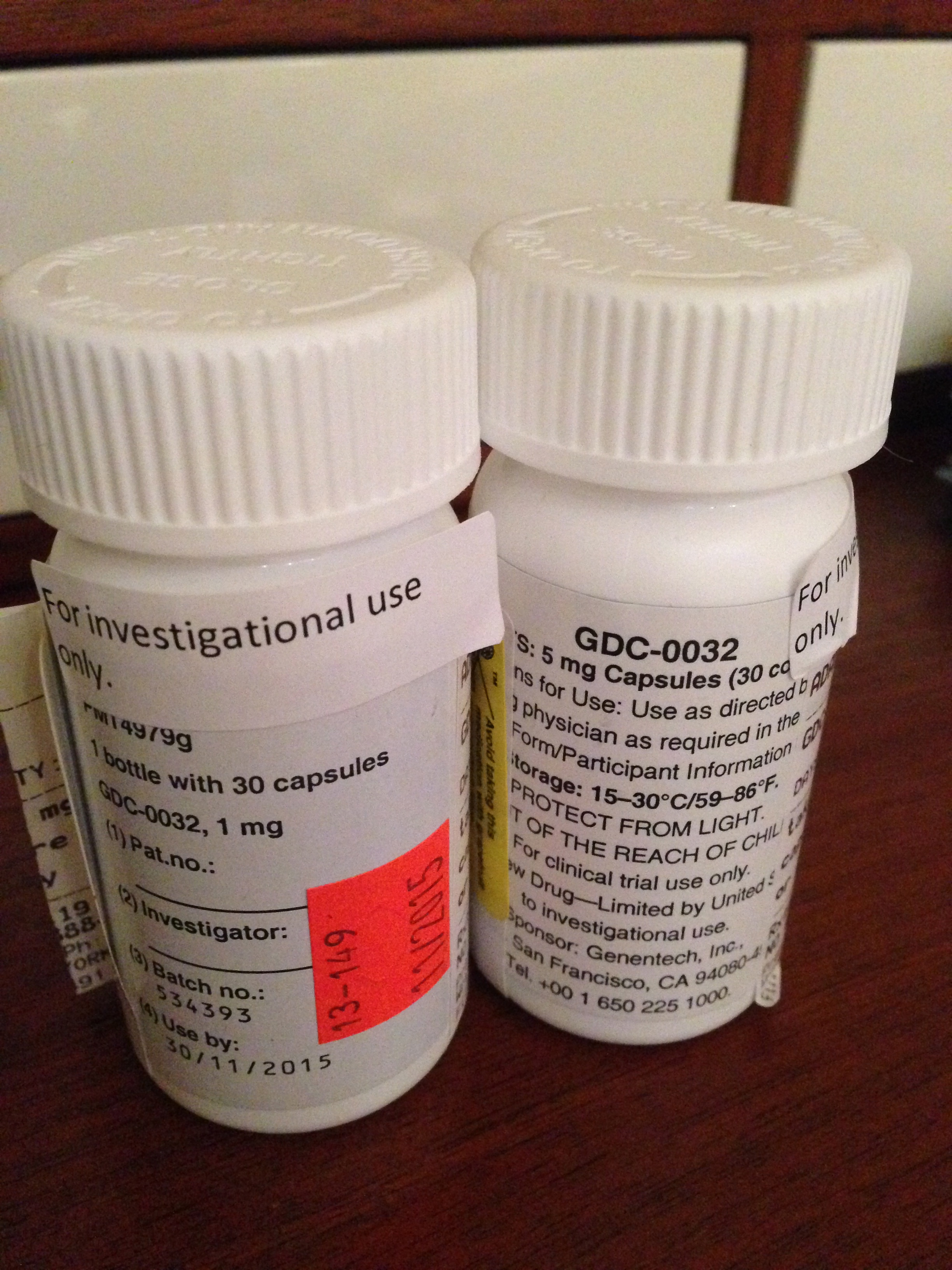
 No news isn’t always good news. A lot has been happening in the last few days. On Tuesday they successfully drained 2 liters from my left pleural space after the unfortunate failed attempt last Friday. There is still about one liter remaining in there (the doctor can only safely remove about 1.5 liters at a time). Think about that: two liters. The size of a soda bottle… a few pounds. From one side. It’s astounding how much space and weight that is. Those are the actual bottles of fluid in the photo.
No news isn’t always good news. A lot has been happening in the last few days. On Tuesday they successfully drained 2 liters from my left pleural space after the unfortunate failed attempt last Friday. There is still about one liter remaining in there (the doctor can only safely remove about 1.5 liters at a time). Think about that: two liters. The size of a soda bottle… a few pounds. From one side. It’s astounding how much space and weight that is. Those are the actual bottles of fluid in the photo.
Everyone kept telling me how great I would feel after the thoracentesis. I did feel like I was breathing easier, but I didn’t feel great. In fact, I had quite a bit of pain. They checked for an air leak by x-ray as they always do after this procedure. There were no visible complications. But there was still tremendous pain starting that day and increasing into the next. It was more than the pain from the reinflation of a lung that had been compressed by half its size. But exactly what it was we weren’t sure.
By Thursday when I had to go back to Sloan-Kettering for my PET scan, echocardiogram, and EKG I was in agony. One of the doctors I met with could see how much pain I was in and prescribed some narcotics. I can’t take anti-inflammatories because I am having a liver biopsy next week and they put patients at risk for bleeding. I am so grateful a doctor seeing me about paperwork reached out to offer assistance and relief.
My father met me in the city. After I completed the required tests he drove me home. I can’t think of anyone better qualified to keep an eye on me than a retired cardiothoracic surgeon. Unfortunately, the pain continued. In all likelihood it is a combination of the cancer causing inflammation in the pleura and some nerve inflammation now that some of that fluid is gone and the lung is reinflated. It’s really all conjecture. We will see if the scans and tests reveal any additional information.
Oxycodone couldn’t keep the pain under control so yesterday I had to combine it with a Fentanyl patch. This duo is definitely helping me more; I’m still in pain but it’s more manageable today (Sunday). Each of these patches lasts for 72 hours and will deliver a constant stream of medication to me. I am pretty much bedridden.
It’s looking like Tuesday (New Year’s Eve) will unfortunately be a tough day. I was already scheduled to have a liver biopsy (This is not to check for malignancies; we already know there are metastases here. This procedure will be for repeated genomic sequencing analysis and other testing to make the best choices about chemotherapy and future clinical trials). Now, given all of the events this week, the team has decided that I need to have a PleurX catheter put in. This is a drainage system that will allow me to remove excess pleural fluid at home rather than having to have it tapped with a needle each time it builds up. The catheter will stay in place only as long as I need it, which will be as soon as treatment starts working and the fluid stops being produced in such copious amounts. I assume this will be at least a few weeks.
Having these two procedures and pain control issues means I will need to stay overnight in the hospital for observation. It’s amazing the lengths some people will go to to be in NYC for New Year’s Eve fireworks, isn’t it? Maybe Anderson Cooper will swing by while I’m recovering.
Once we see the results of all of the tests I’ve had and have these two procedures behind me, we will re-assess the plan to start the second clinical trial on Thursday. The most important immediate tasks at this point are to treat the two symptoms and get my breathing and pain under control. Immediately after that we go to work on the metastases to stop the problems at their source.
Thank you for all of the support I’ve had over the last few days including local friends who have been so kind and some friends who came from quite a distance to keep me company this weekend. I’m just putting one foot in front of the other and doing everything I can to gather all of the information I need to make a decision about what the best next step is.
Of course, as much as I can, I’ll keep you posted. Twitter is always the best way to keep up to date on daily happenings. It’s a lot easier for me to get quick bursts of info out in that medium. So many have asked: I have all of the help that I need and respectfully ask for no visitors or gifts during this time.
I would like to wish you all a happy and healthy 2014 if I don’t post again here before we all ring it in.
December 23rd, 2013 §
 For three days I’ve been mostly bedridden. During two days of sixty degree weather I didn’t make it out of the front door. What I believe is a virus sidelined me for the weekend and today (Monday) I’m still trying to get strength back. Thankfully I think it’s my immune system making me the target; no one else in the family has gotten it.
For three days I’ve been mostly bedridden. During two days of sixty degree weather I didn’t make it out of the front door. What I believe is a virus sidelined me for the weekend and today (Monday) I’m still trying to get strength back. Thankfully I think it’s my immune system making me the target; no one else in the family has gotten it.
Tomorrow I will go back to Sloan-Kettering for another attempt at a thoracentesis. I have had many people ask more about the process and what it is. This was a very good summary with a graphic. It kind of gives me the willies (does anyone even say “willies” anymore?) to look at that.
When even television seems too much,
And hours go by staring out the window.
I listen to the sounds of my children playing,
I hear life go on without me.
It was a day like this that I wrote the lyrics to the song “Six Minutes,”
A day I wished for the time to go. Just go by faster.
But as on that day,
Today I am aware that these are the days I’m fighting for.
If I didn’t want them I wouldn’t be doing all of this.
I know that this is a tough day. Tomorrow will be one, too.
But I also know that someday, hopefully long from now, it will count as a good day, a great day.
And that realization scares me too.
I spoke with a patient care representative at Sloan about some of the mistakes that were made on Friday. I told her my story and we talked about some ways she could follow up. I told her I wasn’t angry, I know mistakes happen, but I thought there were ways to try to make sure these things didn’t happen again. At the end she gave me her contact information. I said, “I love my doctors and the care I get. But there are always ways to improve. I appreciate the chance to give those suggestions to someone who can do something about them.”
Then I started laughing. “You know, I hope to be calling you with suggestions for many years to come. That will mean I’m still here, trying to help patients get better care and trying to help doctors and nurses provide it.” She started laughing too. “You know, I really like that perspective. I’m not sure I’ve ever heard it put that way. I like thinking about more suggestions as meaning more time.” We thanked each other and hung up.
And I thought about it.
Everything is an equation now.
Everything is a calculation.
Everything has a cost.
I try to balance risks.
I study statistics and results.
But in each equation I calculate, the result is always time.
Nothing is more valuable than time that I am able to enjoy the world and those around me.
December 21st, 2013 §
 When I was growing up and there was a particularly tough day my mom would use the expression, “Mama said there’d be days like this.”
When I was growing up and there was a particularly tough day my mom would use the expression, “Mama said there’d be days like this.”
Yesterday was one of those days.
My husband and I left the house before dawn. At about 8 AM I started my appointments. First was a physical exam with vitals taken and a review of symptoms. I met a new oncologist who was filling in while so many of the doctors were away (Friday of a holiday getaway week). We arranged this match because she is the Principal Investigator on a new clinical trial the team has been discussing as a good fit for me. As regular readers know, in my last post I explained that my cancer has progressed in some spots (stable in others) so we need to try to find something better now.
We reviewed my scan results and what she and my regular onocologist think we should do next. A slot in a new trial opened this week and it seems to be a reasonable next step to try another non-chemotherapy method. I’m going to save the details of that study for a later post but for those of you who know and understand the jargon, this one involves a Novartis drug called LEE-011 which is a CDK 4/6 inhibitor in combination with an anti-hormonal agent. This clinical trial is what I’m signing up for next.
The protocol for this drug is very challenging. It involves many trips to the city, especially in the first month where it will be once or twice a week, sometimes just for a blood draw. Some of those visits will be 8 hour sessions where blood is taken a few times to check drug levels in the blood before and after taking the pills. None of the blood draws can be done near my house since the conditions and testing all must be carefully controlled as part of the study. I’ll enumerate side effects and other details in a later post but this one looks to affect me more in daily functioning than I’ve had to deal with in the last few months. I’m definitely nervous.
We talked for a long time about the study. I had already gotten word from my oncologist about her own recommendation. I signed consent forms. I scheduled the necessary tests. They require a CT scan (I just did one, though it falls 2 days outside the testing window. We should be able to get an exemption for that so that I don’t need to redo it). I will need a PET scan, likely need a repeat bone scan, an echocardiogram (this drug can have cardiac side effects), an electrocardiogram, blood test, urine test and, (rats!) a liver biopsy. All of these must be completed in the next two weeks during my “washout period” (interval of time where you are not taking any chemotherapy agents and so you are starting with a clean slate to measure effects in a new clinical trial). Of course, the holidays are not an easy time to accomplish all of these.
I then went to get chest x-rays to monitor my pleural effusion (fluid in the sac around my lungs that makes breathing difficult). After those x-rays and fasting until almost noon I had 40 minutes to finally grab a quick bite. Then I went to the main hospital to meet with a pulmonary physician to decide what to do about the pleural effusion and find out how bad it actually is.
I had a full medical history and symptom assessment with a nurse and then met my new pulmonary doctor. He told me that my left lung is compressed to about 50% of its usual size from the fluid that is there. He estimated 1.5 liters of fluid have accumulated. He said it “layered” on x-ray which means it’s still flowing and therefore would be easier to extract. We decided to do a procedure called a thoracentesis to drain it. One of my morning blood tests that had to do with clotting had come back high, something that would mean we couldn’t do the test. We figured out it had been drawn from my port, which should never be done for clotting tests because they use an anti-clotting liquid called Heparin to flush the port each time and that would lead to inaccurate results.
Through a lab snafu it took 2.5 hours to get the new results rather than 40 minutes. By the time we finally had the all-clear to proceed it was about 5 PM. I still had barely eaten or had anything to drink. For the draining they sit you on a table with your feet dangling and have you bend over a stand for support. It is very much like having an epidural placed. They use local anesthetic to numb the skin and then stick a needle between your ribs, insert a catheter and vacuum extract the fluid (which should take about 10-15 minutes). The doctor got the catheter in, got a small sample of fluid going and…
My blood pressure plummeted. My heart rate dropped. I got hot and woozy and clammy. Yup, I passed out. They had to remove the drain and get me on oxygen and lay me down. I revived quickly, but we could not continue. So, I have the pain from the needle in my back but nothing to show for it. I will now have to go back on Christmas Eve to try again (fully hydrated and fed, hopefully this will be the key). I was obviously disappointed and emotional by this point. I had to go get the X-ray you need to confirm that no damage was done by the needle, and we made a train that got us home at 8 PM. It was a long exhausting day without too much to show for it in terms of relief.
It’s hard not to feel defeated on some of these long days when it just seems the mountain is so big to climb. Right now we are making a change to try to get better results in controlling cancer progression. I won’t be able to to travel for the holidays anyway, but now I will be spending time in hospitals rather than resting at home and taking a break. Cancer doesn’t give a damn about Christmas. Or families. Or anything that matters to me. But my doctors do. And they continue to show caring and concern and work so hard to try to make things better. Without that help and support this would be so much harder. Even when mistakes happen (and yesterday there were quite a few with blood draws and lab tests and so on), every doctor apologized. I definitely shed tears many times yesterday out of frustration, which doesn’t happen too often.
As I waited for my results I watched the office staff exchanging gifts, talking about holiday parties and Christmas cookies. One by one they packed up their belongings and turned out the desk lights. I was the last patient left in that department. That was hard. But I also know that I got to walk out of the hospital last night. I still got to go home and sleep in my own bed. And when I got home I made it just in time to hug my children and see Tristan’s artwork, all sparkly and smile-inducing. He asked me at bedtime why I couldn’t go on vacation with the rest of the family again this year. I explained to him that altitude makes it harder for me to breathe. The air is thin, and I would not feel well. I asked if he understood. “Yes, but I am still sad you can’t come.” “Me too, honey. Me too.”
I’m going to need to dig deep over the next 6 weeks. I’m going to need to ask for help with child care and logistics while I’m recovering from procedures and having so many trips to Sloan-Kettering. That’s not easy either. I find it very hard when I feel that I’ve not been strong enough, or that I’ve complained about the way a hard day has gone. I know it’s normal to need to just cry and complain and say to the cold night-time sky, “This isn’t fair. This isn’t how it is supposed to be.” Sometimes you just need to vent, though.
I need to be strong for the next few days and what they will bring. I want to make the holidays joyous for my family to the degree I can. These are the tasks that make me feel like me. The family shopping is done, the teachers’ gifts distributed, the tips for those who help during the year have been handed out, the holiday cards sent. These are the things that I know I could get a “pass” on. But they are the things I value. I will always try to show my gratitude to others.
Yes, Mama said there’d be days like this. But tomorrow is another day. And I don’t lose hope that it will be better.
December 18th, 2013 §
 “This one has to work,” she says, “It just has to.”
“This one has to work,” she says, “It just has to.”
These are the words my phlebotomist says to me every time I see her. She says it strongly, willing it to be so.
I wish it were that easy. If wanting it could make it so… all of the people who send their support in prayers, thoughts, hopes, vibes, whatever it is they hope will help… all of those would work. And yet, here we are. Through no fault of theirs, or mine.
It is important to see the larger picture here, aside from my own life. It is important for everyone reading this blogpost to know that despite all of the hype and exclamation points and strong language about a cure or the promise of successful long-term targeted agents for metastatic breast cancer so that it can be more like a “chronic disease,” we are not there yet. The number who can live like that are the minority. Most live in this life and death game of Whack-a-Mole that I do now: metastases (“mets”) pop up, and you try to bash them back down but as you do they pop up somewhere else.
The state of metastatic breast cancer care is that you can’t just test your breast cancer, look on a chart to find the drug that will work and always shut it down. Metastatic breast cancer has eluded this formula so far. We don’t have drugs yet to even target every mutation. And we don’t know which inhibitors work. Most work best in combination with other treatments and we have to have clinical trials to test all of those options. All of those things take something those of us living with MBC don’t necessarily have: the luxury of time. In my case, I have a type of mutation called Pi3k-alpha in my cancer. I took an investigational drug that was a Pi3k-alpha inhibitor (along with another drug). On paper it should have worked. It was the most advanced type of targeted treatment I could get for that mutation.
Cancer is complicated. It has multiple pathways to get fuel. Block one? It finds another. And even when you have a drug that shows results in mice or in a few other people, you don’t know if it will work for you. There are too many variables, too many drivers of cancer in complicated feedback loops.
You can see where this is going. I have come out on the wrong end of the equation yet again. The trial drug combination did not work.
I’m no longer continuing on the clinical trial of GDC-0032 and Faslodex that I’ve been on for 8 weeks. The trial is required to drop me and we (my team and I) agree it’s not wise to stay anyway.
My CT scan showed stability in my disease in the bones, lymph nodes and lung nodules. That’s good.
But we have other more serious concerns now. The breathing problems I was having we knew were due to a pleural effusion which initially worsened 6-8 weeks ago and then seemed to improve about a month ago. I have still been aware of breathing issues throughout the day but it hasn’t had too much impact on daily functioning so I have just pushed through.
We now have confirmation that the pleural effusion is larger than in the last scan. The fluid that is causing the trouble is from metastases to the pleura (not to be confused with metastases to the actual lungs, the pleura is the sac that the lungs sit in. They usually have a trace amount of fluid present. This amount is a lot more. The fluid associated with the cancer has settled in the left lower lobe and has displaced the lung upward). In plain terms, there is cancer in the pleura that is producing fluid that builds up in that normally thin sac beyond what can be drained by the normal body process.
Additionally, my liver is now affected as well, unfortunately. There are mulitiple lesions that are metastases as well. This is obviously something I was hoping to avoid for a while longer.
The nature of metastatic breast cancer is that you don’t know how fast things will move or where the cancer cells will settle and thrive. They like the environment of soft tissues (liver, brain, etc.) so these developments are not surprising nor what I want to be hearing.
We need to get aggressive in a new way now. Anti-hormonal agents and inhibitors have not been working for me even though on paper they “should.” Treatments that logically should work might not. And that’s why I get angry when some very visible people in breast cancer care want to keep talking about how “close” we are to personalized treatments and even cures. The research has yet to support that idea. In fact, the latest research has repeatedly shown how complex the interactions are. We now know there are more than 30 subtypes of breast cancer. And even those subtypes don’t always respond alike to treatments.
Cancer is wily. And I hope I’m wrong about how far away we are from true leaps and bounds in MBC care. But I know I won’t see it in my lifetime. For how many decades now have we been hearing about those “breakthroughs” and “miracle drugs”? Yes, they’ve come in some cancers. But not MBC. Reporters and health care professionals in the public eye need to monitor how they spin info about the current state of metastatic breast cancer treatments. Let’s not send the message out about how “close” we are to a cure when there isn’t research to back it up. Let’s not send a falsely reassuring message out there that metastatic breast cancer doesn’t need much attention because soon we’ll be able to make it like a chronic disease anyway. Until we have actually done that, we must push full steam ahead and not encourage complacency in research.
Stepping off my soapbox to come back down to my life, what does that mean for me now? We must choose a new game plan. The one we talked about only days ago doesn’t seem the best option anymore (that’s one reason I don’t take the time to go into my plan B here when it’s still a hypothetical. You always have to be ready to adjust based on new information). We’re huddling and tossing around some options. I should know by Friday when I go back to my last clinic appointment on the trial. In all likelihood I’ll be going to traditional chemotherapy.
For now, it’s hard news to hear, especially at the holidays. I was originally diagnosed with early breast cancer on December 20, 2006. That anniversary approaches. I search for the beauty each day. I make myself find it. I won’t give up these days even when they are so hard. Today as I drove the kids to school the full moon sat above the horizon. It was beautiful in the blue sky after our gray day of snow and rain yesterday. We all looked at it. And I was glad to be able to see it with them.
As many of you already know, my first tweet of each day is a mantra I’ve written: “Find a bit of beauty in the world today. Share it. If you can’t find it, create it. Some days this may be hard to do. Persevere.” I love to start my day with that saying each morning. It centers me. And so many have responded that they like it too.
This news is not good. But as always, I go forward. As I’ve written elsewhere:
Cellular biology is King,
But paired to that fateful ruler I shall be a rebellious, argumentative Queen.
……………………..
One side note: with the popularity of my Twitter feed and the New York Times feature, my volume of email has soared in the past few months. I get so much mail, often with long stories and also requests for advice and guidance about cancer treatment and coping. I am so sorry to say that I cannot always respond to these letters. I hope everyone understands this. I am flattered but the time it takes to fully respond would be like writing a blogpost to each person. If the requests are easy, I try to answer as many as I can. I read every email that comes in and every comment on the blogposts. Any answers to emails come only from me. So I just am hoping that everyone understands that during these turbulent times, I won’t be able to reply to individual requests for advice and care. Thank you for understanding.
December 12th, 2013 §
 Monday morning was an icy, rainy mess. I left the house before dawn, hitching a ride into NYC with Clarke as he drove to work. He dropped me right at the hospital because the weather was so nasty. I only had a short wait until the offices opened at 7:30 and started my first meeting around 8:00.
Monday morning was an icy, rainy mess. I left the house before dawn, hitching a ride into NYC with Clarke as he drove to work. He dropped me right at the hospital because the weather was so nasty. I only had a short wait until the offices opened at 7:30 and started my first meeting around 8:00.
Before each meeting with the Principal Investigator on the trial (an oncologist) I usually meet with a research nurse. On Monday I had the added pleasure of meeting with the Fellow assigned to this trial. She is a fabulous doctor: thorough, curious, caring. We spent more than 45 minutes going over a checklist of symptoms we must review at each appointment. I need to answer if I am having any of those symptoms, describe them in detail, and rate if they are better or worse than at the last visit. Then we discuss what to do to help alleviate the symptoms. Certain medications are allowed and others are not because they could conflict with the investigational drug.
At this visit my main issues were muscle pain in my back, fatigue, occasional bone pain in my collarbone, continued loss of appetite (though my weight has stabilized), occasional shortness of breath, dry skin and cracked heels, and some minor GI issues. My blood pressure and heart rate are elevated. My pleural effusion has stayed at the reduced level, fluid continues just in the lower left lung lobe.
In general, I feel quite good on the combination of GDC-0032 and Fulvestrant. I’m quite happy with my current quality of life on the combo especially compared to other options like IV chemo. I hope that it will continue. I have historically tolerated targeted therapies very well. I have not had any issues so far with mouth sores, rashes, or serious GI issues which are some of the more common side effects with the investigational drug.
I was able to ask all of my questions, most having to do with the coming two weeks. Next week is a big milestone: I will have my first CT scan and that will be the basis for determining if I can continue in this clinical trial. At least two radiologists will examine the CT. One radiologist from the hospital will read the images, while a second, separate radiologist assigned to the trial will make his/her own determination as to how much disease there is compared to the baseline CT 7 weeks ago. If the cancer metastases are considered stable or decreased, I will continue in the trial. If the cancer has progressed (grown) by 20% or more, I will need to stop taking the drugs and be removed from this trial. There are defined days that are the days I must have this scan done so that all of us taking part in the trial are assessed at comparable points in treatment.
Next I met with the Principal Investigator on the trial. This is the oncologist who is the point person for the trial and supervises all of the patients in the trial at Memorial Sloan-Kettering. We reviewed how I am doing in general, what the plan is for the coming 2 weeks, and discussed bloodwork. I told her that am anxious to hear how the other people enrolled in the study nationally are doing. Because we all started within a few weeks of each other, there aren’t many reports yet.
Because I have completed my loading doses of Fulvestrant (an extra dose of the drug is required in the first month of treatment), I did not have to get those injections this week. That was a treat. I will now receive the two injections monthly.
My medication diary documenting the time I stop eating each night and the time I take my medication in the morning was checked as were my pill quantities. I scheduled my next visit (adjusted a few days earlier because of holiday schedules there, I have a +/- 3 day window for the appointments now) and headed up to the third floor to have my blood drawn.
My port incisions are healing beautifully. I’ve toyed with posting a photo of what it looks like but haven’t decided about that yet. The nurse and I donned the requisite masks for port access and the blood draw was easy. I was then allowed to take my GDC pills and start the clock on the 60 minutes until I could eat and drink (I must always wait one hour after taking them). I left the hospital about 3 hours after I arrived.
We’ve been watching my tumor markers and aren’t quite sure what to make of them. They’ve been rising a lot in the past month but I am also getting varied results from my two testing sites. Of course, the key piece of data to look at is the scan. But it’s been a challenging few weeks emotionally as I see where the markers are, watch them rise, and wait for the scan to tell me what’s truly going on inside by body. In a few days I’ll have answers. And then I’ll either be continuing on the trial for another two months or moving on to plan B (which my team and I have already identified).
I continually try to bring my focus back to the distinction between worrying and planning. Worrying is anticipatory. The way I look at it is that worrying is spending time thinking about things that may or may not be/come true. Planning is taking strategic action to set things in place and control things that I can control in the midst of so much uncertainty.
Having a backup plan or a next step if the scan brings bad news next week is planning. It means if this trial isn’t working I know what I will do next and make sure those steps are in place so I’m not suddenly reeling and trying to cobble together a plan. But worrying about the results next week won’t do me any good. The cancer is doing what it is doing. These drugs are either working or they are not. And my sadness or frustration about that won’t change the reality of the cellular processes.
And so I have been quieter this week, choosing carefully how to spend my time. I’m searching for joy each and every day and finding beauty in the small moments: our dog Lucy playing in the first snowfall of the season, Christmas shopping with Paige last weekend, puzzling through math homework with Tristan, Colin and I getting haircuts together and going Lego shopping.
We hug a lot.
We say “I love you” a lot.
We always have done this.
But now I hold on for an extra second each time and I squeeze just a little tighter.
………………………………….
For those readers new to my posts about this clinical trial, you can see my reports about Cycle 1, Day 1 here and Cycle 1, Day 16 here and my port placement and Cycle 2, Day 1 here.



 Link to Twitter
Link to Twitter