October 22nd, 2014 §
 The past few weeks have been some of the most challenging this year. By the time you read this I will have had my third Navelbine infusion. Unfortunately, we do not have any evidence so far that it is working. Each chemotherapy that I try at this point only has about a 30% chance of working even for a short period of time.
The past few weeks have been some of the most challenging this year. By the time you read this I will have had my third Navelbine infusion. Unfortunately, we do not have any evidence so far that it is working. Each chemotherapy that I try at this point only has about a 30% chance of working even for a short period of time.
For now, we anxiously wait. But that waiting means that the cancer is progressing. Increased fatigue, pain, nausea, weight loss, shortness of breath and weakness are my companions right now. I do have my team helping me manage these side effects, but there is trial and error involved. Also, at this point an increased cancer load is part of the problem. The only thing that will truly help that is to find a systemic therapy that works, and let it do its thing. For that reason I haven’t been able to post as often as I wanted this week.
I do want to share that the book auction to raise money for my metastatic research fund at Memorial Sloan-Kettering is now live, and it runs through October 24th. This is an exciting event. You can bid by posting a comment including the amount of your bid below the photo of the box you want (you must live in the USA to participate). All proceeds fund research and do NOT go to my personal medical care. Boxes of signed books have been donated by authors and then collected and curated by Erika Robuck. You can click here to go to the Facebook page and then scroll down to see all of the boxes.
Last year the event raised over $4000 and we are on track to blow that out of the water. If you want to donate directly to the research fund but don’t want to participate in the auction, don’t have Facebook, or don’t want to deal with Facebook, please feel free to go here. Donations of any amount are so appreciated.
For today’s October re-post I’ve chosen one of my first pieces, one that readers ask for again and again. I have decided to revise it here, now that my diagnosis has changed. I’m keeping the original post online, though, and you can see that here.
………………………………………….
I wish I had the energy of my youth.
I wish I had the body.
I wish I had the fearlessness, the spunk, the drive.
I wish I could have a conversation with that young girl,
bright-eyed and full of wonder.
I wish I could tell her what lay ahead.
I wish I could tell her to gather strength, and wisdom, and patience like a squirrel gathering acorns for the winter.
“Save those things up,” I’d say, “you are going to need them… every last bit.”
I wish I could share the perspective I’ve gained along with all of the love.
But I can’t go back to that time,
I can’t go back to that place.
I can’t rewrite what’s happened,
I can’t do it all again.
My first diagnosis with breast cancer took its toll on me and I was quite sure I would never, ever be the same.
I had no way to know then that “never, ever the same” would mean something worse, something fateful, a juggernaut.
I told myself “they’re only breasts.”
I said, “I don’t need ovaries, I’m done having children.”
But that obscured the truth.
The truth is that it did matter,
They do matter.
They said my uterus was atrophied.
It almost sounded funny when they said it.
“Who cares? What does that matter?”
It did. It does. It will.
At the time, to get rid of all hormones was thought to give me a better chance at avoiding a recurrence, but there was a price to be paid.
No estrogen mattered more than I ever thought it could.
It felt worse than taking injections to suppress my ovaries, worse than taking Tamoxifen.
Those were easy.
I had no clue what was ahead.
I wore the skirt, I put the makeup on, I walked the walk.
But I did not feel like a woman anymore.
I most certainly do not feel like much of one now.
Make no mistake, I am proud of what this body has done for me.
My three children top the list.
But now I must focus on some of its cells,
now malignant,
throughout this body,
growing at a horrific pace.
My body has now become a personal science experiment.
Sometimes, when things are going well, you could look at me and have no earthly clue.
You see,
Beneath the pretty lies ugly,
the ugly truth of cancer
and what it has taken from me.
While some may be able to go on,
move on,
forget,
I cannot.
My body will not let me.
These things are not tied with a pink ribbon.
These things last longer than a month.
This is part of awareness.
This is just a part of what breast cancer can do.
This is just a part of what breast cancer has done to me.
This is part of what can happen
Even with early detection and treatment.
This is what can happen even years later.
This is why people should not prematurely claim victory.
This is why you are not necessarily safe.
This is what breast cancer could do to you.
This is how what some think they have “beaten” or “bid goodbye to” can still
kill.
This is what it will do to me.
October 17th, 2014 §
My last post (“The Hardest Conversation”) showed you what a conversation with my teen daughter was like when we talked about my diagnosis of metastatic breast cancer in 2012. Today I wanted to share a conversation with my youngest child (now 8) that happened last year so you can see the variation in what their concerns were and how I dealt with each one.
As always, with cancer, age-appropriate explanations are important. Another vital piece of advice I’d like to share is that with all children, but especially young children, it is important to talk more than once about the topic. At the end of the first conversation I recommend asking young children, “Can you tell me what we talked about today?” to see if they have absorbed the most important pieces of information and that these pieces are correct. A day or two later it is always a good idea to ask, “Now that you’ve had time to think about our chat, do you have any questions?”
The following post was written in late 2013 on the eve of the surgery to put my medi-port in.
………………………………………………
 “Why do you have to have surgery tomorrow?” seven year-old Tristan asks from the back seat after we drop off his 11 and 15 year old siblings this morning.
“Why do you have to have surgery tomorrow?” seven year-old Tristan asks from the back seat after we drop off his 11 and 15 year old siblings this morning.
“Because I need to have something put in my body called a port. It’s a little container made of something cool called titanium that lets the doctors put some of my medicines into my body in an easier way.”
“Can you see it?”
“Yes, you will be able to see that there is a lump under my skin, about the size of a quarter. But you will only see the lump. You won’t see the actual thing because that will be inside my body. You know how I have the scar on the front of my neck? It will be like that, here, off to the side, same size scar but with a bump under it.”
“Is it like the bubble I had on my neck when I was a baby?”
“Well, that was a skin tag, so that was a lot smaller. And they were taking that away. This is something they are putting in to help make it easier to get some of my medicines. And you know when you go with me and I have blood taken from my hand? Well now sometimes they will be able to just take it from there instead. So it helps with a few jobs.”
“Will you have it forever or do they take it out when your cancer goes away?”
(Driving the car, trying to keep tears in check, knowing this is a vitally important conversation. I’ve explained this to him before but I know it’s hard for him to understand.)
“Well, honey, remember I had cancer when you were a baby? Well, this time the cancer is different. A lot of the time you can have cancer and the medicines and surgeries make it go away and it stays away for a long, long time. Maybe even forever. Sometimes any cancer cells that might be left go to sleep and just stay that way. Sometimes you have bad luck and they wake up. Mine woke up after six years. And now the cancer cells are in places that I won’t be able to get rid of them all for good. I am always going to have cancer. This time my cancer is the kind that is always going to be here.”
“You’ll always need medicine. And the thing they are putting in?”
“Yes, honey, I will always need medicine for my cancer. And I will probably need to have the port in forever too.”
Long silence.
“I am glad you are asking me questions about it. I want you to always ask me anything. I will try to explain everything to you. I know it’s complicated. It’s complicated even for grownups to understand.”
Long silence.
“Mom, did you know people whose eyes can’t see use the ridges on the sides of coins to tell which one they are holding? So if you have a big coin with ridges that person would know it is a quarter?”
“That makes sense. How did you learn that?”
“At school. And so if it’s smooth you know it’s a nickel or penny. It’s important that they know what coin it is.”
“I think you’re right. That is very clever.”
( I stay quiet waiting to see where he will take the conversation next.)
“Remember when my ear tube fell out and was trapped in my ear and the doctor pulled it out and I got to see it? It was smaller than I thought it would be.”
“Yes, I thought the same thing.”
“I really wanted to see it. I wanted to see what it looked like.”
“Me too.”
“Can you show me a picture of it?”
“Of what?”
“The thing for tomorrow.”
“The port?”
“Yes. Or don’t you know what it will look like?”
“I know what it will look like. Sure, I will show you on the computer after school.”
“Okay.”
“It’s time for school but I am glad we talked about this. I want you to keep asking questions when you don’t understand something. I love you, Tristan. I hope you know how much. I know this is hard for all of us. I wish it were different. But we are going to keep helping each other. And talking about all of this is good. We can do that whenever you want.”
October 15th, 2014 §
 From the time my oldest child, Paige, was born everyone kept telling me, “Just you wait.”
From the time my oldest child, Paige, was born everyone kept telling me, “Just you wait.”
When she made it through the terrible twos without much of a tantrum everyone kept telling me, “Just you wait.”
When she made it through elementary school and a move from NYC without trouble they kept saying, “Just you wait.”
“Just you wait,” they said, “girls are drama. You got lucky before. But the teen years? Oh boy… just you wait.”
Today she prepared me a bowl of soup and brought it up to my bedroom. I was resting after my surgery to remove malignant lymph nodes and tissue for testing yesterday, the room was dark. I invited her to come snuggle with me in the big bed. We’ve never let our children sleep in our bed so they think climbing in is a big treat.
I asked her if she wanted to talk about what was going on, about my news about having metastatic breast cancer. She did.
And so it began: an hour-long talk that started with her first question, “Are you scared?”
She asked questions about genetics and risks of getting cancer to what kind of treatments I might need.
She asked me again, as if to confirm for herself, “It’s not curable, right?”
We talked about my writing, about being public with my health status, about being open and honest with her and her brothers.
I told her that yes, I was scared. I explained that my fear usually comes from the unknown, in this case just how I will respond to treatments. I told her it was okay to be scared. That it’s normal, that sometimes fear makes you brave enough to do things you don’t think you can otherwise do.
I told her that I understood that sickness could be scary, that I didn’t want her to be afraid of me as I got sicker someday. “I would never be afraid of you, Mom. I’m only afraid of cancer,” she said. My heart squeezed and thrashed and the tears flowed.
We talked about her desire to be a doctor, a surgeon. She wanted to know what all of my surgeries and treatments had done. She wanted to know the difference between cancer “stage” and “grade.” We talked about the genetics of breast cancer and discussed the BRCA-1 and 2 genes (which I do not have). We talked about hormones and their role in puberty, menopause, and cancer. She wanted to know why outcomes are so variable. How will we know if treatments are working? I told her about the importance of her monitoring her own health, how hopefully we will have better screenings down the road.
I told her that for now I want her to live her life, for our house to be as normal as it can be for as long as it can be.
I told her she should try to focus on her schoolwork, her sports, and her friends. She told me that I was more important.
I told her that eventually I might need someone to help take care of me. “I will take care of you, Mom. You’ve always taken care of us,” she said.
We talked about her brothers, ages 11 and 6 and how she was going to have to help them. And her dad too. “I’m really good with hospitals and medical things, Mom… I’m just like you.”
She said she liked that I was open about it. That people knew. She thought it was best to be honest and appreciated the offers of support she’d received from friends and adults she knows.
I told her that what we were doing, lying there talking for an hour together about this, was the most important thing we could be doing today. I told her there wasn’t anything more important to me than my family. My job is to help them deal with this. Whatever this is.
I explained that what she needed from me would likely differ from what her brothers need; she is older and each of them would have different needs along the way. It’s my job to figure that out and address it. And my husband’s job now, too. How I take the lead on this will be important.
She asked if that was a lot of pressure, to have so many people reading my words, watching what I was doing. I told her it was. I told her it was my way of trying to help people. The same way that she wants to be a doctor to help others… well, I have always tried to see if I could help in my own way. And the way we talked before about the unknown being what’s scary? Well, my writing here means it’s less mysterious. Knowledge helps. Even if the knowledge is not what you want to hear, knowing is better.
Denial won’t change the course of things, and often makes things worse.
Secrecy is bad. Sharing and supporting are what I champion. And I know that de-mystification is a constant effort. I will continue to teach my children daily. I said I hoped that somewhere in all of this she could see how important science and medicine are in my world. And that if she does decide to be a doctor that is a noble effort. She will make me proud in whatever she does. As will my boys.
The funny thing is how much better I felt after we talked. The conversation was the hardest one I’ve had. The topics are gut-wrenching. But shining the light on them, on this disease, on what happens next, is the only way I know to cope, to help, to keep going.
We talked on and on as I combed my fingers through her long hair. I stroked her smooth, soft cheek. She was giving me strength.
And what I realized about people saying I should just wait because she’s going to eventually act out:
Waiting is a luxury.
Waiting means having time.
And that’s what I want most in this world right now.
October 12th, 2014 §

I make sure my family goes on trips without me now.
It is important that they learn to be without me.
Important that they get time away from here.
Important that they know there can be fun and joy even if I am not with them.
This is what I want.
This is what will be.
It is not easy to be the family of someone who is ill.
I know this is true.
And so I send them away to laugh, to be together, to have fun.
This is what I unselfishly demand.
In April of 2013 we all went to Florida. I didn’t know it would be our last trip together for a while. I could not focus very well. I just knew that life was not the same and it never could be. I had learned about six months earlier that I had metastatic breast cancer. I knew I would never be carefree again. I had intended to stay away from writing for that time, but on this particular day, in this moment, all I could do was realize the agony that was my situation. When I got back to the hotel room I wrote the words that had been in my head.
…………………………………………………
“Floating Away”
 I sit on the beach, feel the sand’s angry texture rub my chemo feet in a way I wish it wouldn’t.
I sit on the beach, feel the sand’s angry texture rub my chemo feet in a way I wish it wouldn’t.
I watch my family in the ocean, turquoise and calm and vast.
My husband flips over, face in the water, takes some strokes out to sea.
His movement is graceful, effortless, just as it was the when I met him 22 years ago.
He was a sprinter on the college swim team then,
and while he laughs and says it doesn’t feel effortless anymore,
nor perhaps fast,
it does not matter.
In my mind’s eye he is that young man,
swimming fast,
joking with his team,
coming over to the stands to talk to me while chewing on the strap of his racing goggles.
I fall in love with him again every time I see him swim.
My three children float, bobbing in the ocean water.
I can feel the distance between us, it feels like a lifetime.
It is my family in the ocean floating away from me.
I see the quartet, I watch as an outsider.
I do this a lot lately.
I watch them from afar and think how it will be without me.
A new family unit.
Behind the big black sunglasses my tears stream down.
Suddenly Tristan is running from the water to me, across the sand.
He stands, dripping, face beaming.
“I just wanted to tell you I love you, Mama.”
I take his picture.
I capture the sweetness.
I grab him, hug him, feeling the cold ocean water on him, melding it to my hot skin.
I murmur to him what a sweet boy he is, that he must never lose that.
I send him back to the ocean, away, so I can cry harder.
By the time they return to shore I’ll have myself composed.
But my oldest immediately senses something amiss.
She mouths to me, “Are you okay?” and pantomimes tears rolling down her cheeks.
Yes, I nod.
I walk to the water’s edge to prove it.
October 10th, 2014 §
 When I die don’t think you’ve lost me.
When I die don’t think you’ve lost me.
I’ll be right there with you, living on in the memories we have made.
When I die don’t say I “fought a battle.” Or “lost a battle.” Or “succumbed.”
Don’t make it sound like I didn’t try hard enough, or have the right attitude, or that I simply gave up.
When I die don’t say I “passed.”
That sounds like I walked by you in the corridor at school.
When I die tell the world what happened.
Plain and simple.
No euphemisms, no flowery language, no metaphors.
Instead, remember me and let my words live on.
Tell stories of something good I did.
Give my children a kind word. Let them know what they meant to me. That I would have stayed forever if I could.
Don’t try to comfort my children by telling them I’m an angel watching over them from heaven or that I’m in a better place:
There is no better place to me than being here with them.
They have learned about grief and they will learn more.
That is part of it all.
When I die someday just tell the truth:
I lived, I died.
The end.
October 10th, 2014 §
 I’ve been struggling with side effects from the new chemo so I haven’t posted for a few days.
I’ve been struggling with side effects from the new chemo so I haven’t posted for a few days.
I know Al Jazeera Television has been rebroadcasting the episode of “The Stream” that I participated in last year. For those who missed it, I want to make it easy for you to watch. This was a rare event because they gave us a full half hour show to talk about Pinkwashing and Breast Cancer Awareness. Dr. Susan Love, Dr. Gayle Sulik, and I were given time to really talk about issues. I give them credit for allowing a whole show for us. To watch, just click on this link https://thinkorbit.app.box.com/thestream101113 (must watch from a computer not a phone).
The photo is of two of my nieces watching me on TV.
October 8th, 2014 §
 It does not matter how healthy you look. It does not matter if your hair is growing back or you walk a little faster or manage with just one nap a day now.
It does not matter how healthy you look. It does not matter if your hair is growing back or you walk a little faster or manage with just one nap a day now.
It does not matter if any of those things are true, your cancer can be worsening.
As I have described here before, metastatic breast cancer is characterized by resistance to therapies. If a treatment works in the first place (and according to my oncologist, most have about a 30% chance of initial success), the cancer will almost certainly become resistant to it and it will cease working. This resistance will happen time after time. This has happened numerous times to me already. I have had some treatments not work at all (Taxol, Fulvestrant+clinical trial drug GDC-0032) while others worked for a few months and then would not work any longer (Xeloda, Aromasin+Afinitor) .
Once again, this resistance has happened. Carboplatin and Gemzar did their work starting in March and did it well, bringing me back from a very dark place this Spring. After 9 complete cycles, though, they are no longer working. It is time to move on.
Moving on is scary. It means being in freefall as we use educated guesswork to decide what agent(s) to try next.
The good news is that I was officially approved to receive palbociclib from Pfizer under their expanded access (compassionate use) program. I will be able to get this drug before it receives final approval by the FDA and therefore before it is on the market sometime in the next year. There is no guarantee this drug will work (alone or in combination with other drugs that are on the market already). It is just one more thing to try.
There are still final bureaucratic hoops to jump through, though, and I won’t have it for at least a few more weeks. This presents a problem: I need a new therapy now. I cannot safely be without treatment for that period of time. It also is best for me to be in a state of control when I start it; the higher a cancer load I carry the harder it would be if what the drug does is provide stability rather than cancer regression. Stability is considered success in metastatic breast cancer drugs. Just keeping things the same, preventing cancer progression, is good. This is considered “success” in using a drug for metastatic breast cancer. However, if you start at a very high cancer load, that stability may be quite intolerable. My oncologist and I feel it is best to have that load brought down (not just held steady), and we don’t know if this drug is a workhorse like that. We can’t count on it to be.
I’ve known for the last week that things were probably over for this chemo. We had tried a higher dose of both drugs already without success. I adjusted to the news over the weekend and yesterday I started on a new chemotherapy regimen. Navelbine is given through my port as an IV “push”; it’s just one syringeful that is given in about 30 seconds. Having a port is really helpful for this one because it is very irritating to veins if you do not have a medi-port implanted in your chest like I do (the port is completely under my skin, it is a lump about the size of a nickel and is accessed with a special needle by the nurses. They can take blood from it, give medication and chemo through it the way you would with an IV except you don’t have to use an arm vein). We are initially planning on a schedule of two weeks on, one week off, but that may change as we go. And of course, if it isn’t working, we’ll have to try something else.
I’m having some other problems now that the cancer is growing so that has been a challenge. Side effects don’t just stop the minute you stop taking a drug. And moving right on to another one means there is no break. It is what is needed though. The good thing is that if you find something that works (like the Carboplatin and Gemzar did for me), they can do astounding things to kill the growing cancer and bring it back under control.
Metastatic breast cancer is like Whack-a-Mole: cancer pops up in places and then can often be whacked back down. If you’re lucky you can play this game for a little while as it takes up residence in different bones and organs. We’ll see how successful we are this time. This is always the hardest time for me mentally: living with the uncertainty of trying to find a new regimen, trying to find something that works, knowing right now there is nothing.
But this is the choice I have made in choosing to treat my cancer. That is the nature of this disease. These are not heroic measures. This is what treating metastatic breast cancer is.
And so we go… onward.
October 7th, 2014 §
 There’s salt on my blue jeans
There’s salt on my blue jeans
And rain left in my hair.
There is a spot of dirt behind his left ear
And mud on his shoes.
I don’t wipe the spot of dirt off.
I stare at it throughout the drive.
I think of when he was a baby, a toddler, a boy.
Now he approaches manhood,
A time when most young men would pull away.
He does not.
He still hugs me in public.
He tells me he loves me.
He doesn’t mind if anyone hears me tell him the same.
He is still mine for a little while longer.
As I contemplate the dirty spot,
I hear the words.
They write themselves
As they often do.
The salt, the dirt, the refrain.
“There is so much left to do.”
It is a track stuck on repeat.
Every moment of my life now it plays.
I showed him a better hamburger today,
He will remember that.
I reminded him about bringing dry socks to the game.
I am quite sure he will forget about that.
I can’t help but smile every time he looks my way.
Or waves from the mound.
During the delay he caught rain in a water bottle,
Shrugged his shoulders when I caught his eye.
He beamed his impish grin.
Later he asks me, “Do you need help?”
He thanks me for coming to his game.
He always thanks me.
He knows.
The salt is gone from my jeans.
The rain in my hair has long since dried.
The dirt and mud are gone too.
But there is so much left to do.
October 6th, 2014 §
 One of the most common questions I get asked by email is, “Someone I know has been diagnosed with cancer. What can I do?” Today I offer one suggestion. I believe this would make a practical gift for someone who has just been diagnosed and it is a necessity if you are the patient or a caregiver.
One of the most common questions I get asked by email is, “Someone I know has been diagnosed with cancer. What can I do?” Today I offer one suggestion. I believe this would make a practical gift for someone who has just been diagnosed and it is a necessity if you are the patient or a caregiver.
Being organized is one of the best ways to help yourself once you’ve been diagnosed. When you first hear the words, “You have cancer” your head starts to swim. Everything gets foggy, you have to keep convincing yourself it’s true.
But almost immediately decisions need to be made — decisions about doctors, treatments, and surgeries. Often these choices must be made under time constraints. You may be seeing many different doctors for consultations. Medical oncologists, surgical oncologists, radiation oncologists, recontructive surgeons, internists— there are many different voices that you may hear, and they may be conflicting. It’s hard to keep it all straight in the midst of the emotional news. Not only are you likely to be scared, but also you are suddenly thrust into a world with a whole new vocabulary. By the time you are done with it, you will feel you have mastered a second language.
You can help your care and treatment by being organized. You can also have the psychological bonus of feeling that one part of your care is within your control. Especially if you are juggling different specialists and different medical facilities, you must remember that the common factor in all of this is you. It’s your health. It’s your life. I believe it’s important to travel with a binder of information about your medical history and treatment, as well as notes and questions.
This binder will mean that all of your information about your cancer will be in one place. This will be your resource guide. I cannot tell you how many times physicians have asked about my binder and when I was able to instantly produce test results, pathology reports, or other information they needed, they said, “I wish every patient had one of those.”
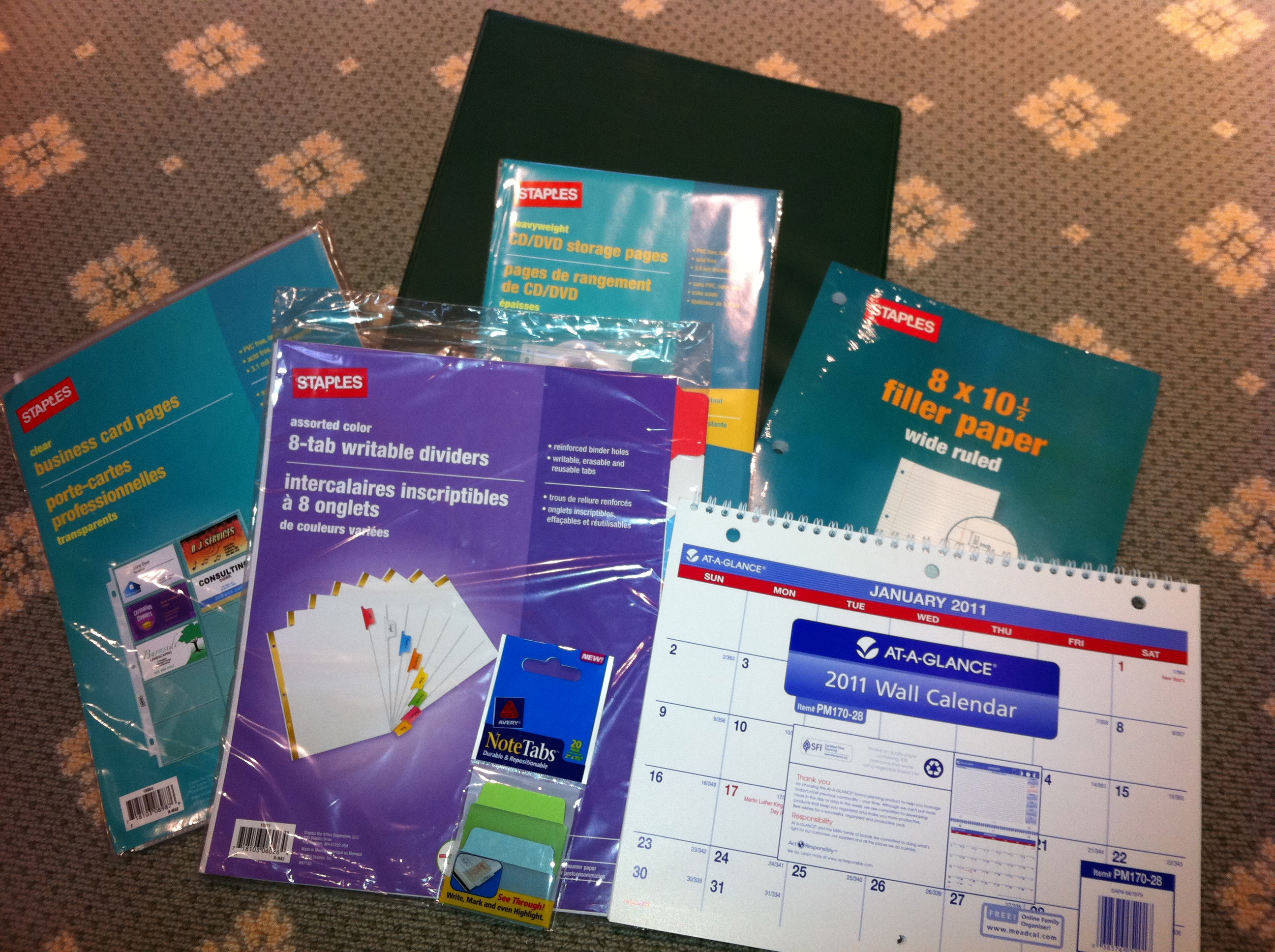
I suggest the following:
A heavy 3-ring binder
I think a 1.5″ binder is a good size to start. This size will allow you to easily access reports and pages and have room for the calendar. It will look big at first but you won’t believe how quickly you will fill it up.
Colored tab dividers
I like these to be erasable. I think 8 is the minimum number you will need. If you have a lot of specialists you will need more. The categories you think you will need at the outset may change. It’s easy to erase and reorganize them. Put the categories you will be accessing the most in the front so you aren’t always having to flip to the back. Once the binder is full it will make a difference.
Some starting categories:
- schedules (dates of appointments you have had, when the next ones are due, and how often you need certain tests done)
- test results/pathology (it’s very important to keep copies of MRI, CT, and pathology reports so that you correctly tell other doctors what your diagnosis is. For example, new patients often confuse “grade” with “stage” of cancer)
- insurance (keep copies of all correspondence, denial of claims, appeal letters, explanations of benefits)
- articles and research (handouts, post-surgical information. Ask if there are any websites your doctor does approve of. My own oncologist said, “Do not read anything about cancer on the internet unless it comes from a source I’ve told you is okay. There’s a lot of misinformation out there.”) Keep your post-surgical instructions, any info given to you about aftercare.
- radiation/chemo (keep records of exactly what you had done, number of sessions, dates, drug names, etc. I also asked how my dose was calculated so I knew exactly how much of each drug I received in total)
- medications (drug names, dates you took them, dosage, side effects). I also keep a list of all of my current medications as a “note” in my iPhone. That way I can just copy it down and won’t forget anything on the list. You should always include any vitamins or supplements you take.
- medical history (write out your own medical history and keep it handy so that when you fill out forms asking for the information you won’t forget anything. As part of it, include any relatives that had cancer. Write out what type it was, how old they were at death, and their cause of death. Also in this section include genetic test results, if relevant)
Loose leaf paper
Perfect for note-taking at appointments, jotting down questions you have for each doctor. You can file them in the appropriate category so when you arrive at a doctor your questions are all in one place.
Business card pages
These are one of my best ideas. At every doctor’s office, ask for a business card.Keep a card from every doctor you visit even if you ultimately decide not to return to them. If you have had any consultation or bloodwork there, you should have a card. That way, you will always have contact information when filling out forms at each doctor’s office. For hospitals, get cards from the radiology department and medical records department so if you need to contact them you will have it. Also, you want contact information for all pathology departments that have seen slides from any biopsy you have had. You may need to contact them to have your slides sent out for a second opinion.
This is also a good place to keep your appointment reminder cards.
CD holders
At CT, MRI or other imaging tests, ask them to burn a CD for your records. Hospitals are used to making copies for patients these days and often don’t charge for it. Keep one copy for yourself of each test that you do not give away. If you need a copy to bring to a physician, get an extra made, don’t give yours up. If you need to get it from medical records from the hospital, do that. You want to know you always have a copy of these images.
Keep a copy of most recent bloodwork (especially during chemo), operative notes from your surgeries (you usually have to ask for these), pathology reports, and radiology reports of interpretations of any test (MRI, CT, mammogram, etc.) you may have had. Pathology reports are vital.
Calendar
I suggest a 3-hole calendar to keep in your binder. This will serve not only to keep all of your appointments in one place but also allow you to put reminders of when you need to have follow-up visits. Sometimes doctor’s offices do not have their schedules set 3, 6, or 12 months in advance. You can put a reminder notice to yourself in the appropriate month to call ahead to check/schedule the appointment. Some people like me prefer to use their phones for this, including reminders.
Similarly you can document when you had certain tests (mammograms, bone density, bloodwork) so you will have the date available. I usually keep a piece of lined paper in the “scheduling” section of my binder that lists by month and year every test/appointment that is due and also every test I’ve had and when I had it.
Sticky note tabs
These can be used to easily identify important papers that you will refer to often, including diagnosis and pathology. These stick on the side of the page and can be removed easily. As your binder fills up, they can be very helpful to identify your most recent bloodwork, for example.
Plastic folder sleeves and sheet protectors
These are clear plastic sleeves that you access from the top. They can be useful for storing prescriptions or small notes that your doctor may give you. The sleeves make them easy to see/find and you won’t lose the small slips of paper. Also a good place to store any lab orders that might be given to you ahead of time.
The above suggestions are a good working start to being organized during your cancer treatment. If you want to do something for a friend who is newly diagnosed, go out and buy the supplies, organize the binder and give it to your friend. He or she will most likely appreciate being given a ready-made tool to use in the difficult days ahead.
I also believe a modified version is equally useful for diagnoses other than cancer. When our youngest son was born with defects in his spine and hands it took many specialists and lots of tests to get a correct diagnosis. Having all of his tests and papers in a binder like this was instrumental in keeping his care coordinated. In fact, at his first surgery at The Children’s Hospital of Pennsylvania they gave us a binder to assist in this process. I know some hospitals do this for newly diagnosed patients already.
Maybe my tips will help you or a friend know how to better use the one you already have. You may not need all of these elements depending on the complexity of your case, but I hope you will find some of these suggestions useful.
October 3rd, 2014 §
 It seems like you can’t rank anguish. You shouldn’t be able to “out-suffer” someone. How do you quantify misery?
It seems like you can’t rank anguish. You shouldn’t be able to “out-suffer” someone. How do you quantify misery?
And yet, somehow we do.
“My problems are nowhere near as bad as yours are.”
“I feel terrible complaining to you about it when you are going through so much yourself.”
I hear these types of comments all the time.
I make these types of comments all the time.
Placing ourselves in a hierarchy of pain and suffering serves to ground us; no matter how bad our situation is, there’s comfort in knowing there is always someone who has it worse.
Like being on a really, really long line at the movies or at airport security, as long as there is someone behind you, it somehow seems better.
Hospitals use a pain rating scale: “On a scale of 1 to 10, how bad is your pain?” When our son Colin was in the hospital for 9 days with a ruptured appendix, they asked him to rate his pain. I was intrigued at his difficulty in answering the question. At the time he was 5 years old and didn’t understand what they wanted him to do. Colin didn’t understand the concept of comparing one level of pain to another; His abdomen hurt… that’s all he knew. He used a binary scale to assess his pain: did it hurt or not? As adults we know better: pain is not a yes-or-no question. Rather, there can be levels, ranking, quantification, and comparisons.
These mental exercises are necessary to keep us going through hard times, no matter what type. Before I got cancer, cancer was a “go-to” negative reference point. I mean, how many times had I, and everyone I know, thought or said, “I’ve got health problems, but at least it’s not cancer”?
I had done that a lot.
A benign lump needs to come out? At least it’s not cancer.
A mole needs to be removed? At least it’s not cancer.
My son has hand and neck deformities and a cyst in his spinal column? At least it’s not cancer.
Then one day it was cancer.
So what could I pacify myself with?
At least it’s not terminal.
At least they can remove the body parts the cancer is in.
At least this debilitating treatment will be temporary and I have the possibility of returning to a normal life again.
Then there was the big one: at least it’s happening to me and not my child.
And when I found out that my cancer had metastasized, I could not calm myself with those comforting refrains anymore.
Now it is terminal.
Now they can’t remove the body parts it is in.
Now the debilitating treatments are permanent and I don’t have the possibility of returning to anything close to a normal life again.
I have often said I have hated becoming anyone’s negative reference point. “At least I’m not her” people now often think of me. I always thought that meant they pitied me. I didn’t want that. But now I realize that it is okay for people to be glad they haven’t walked in my shoes– in reality, that’s what I want. I don’t want anyone to be where I have been and where I am; I’d like to be the lightning rod that keeps other people safe. But we all know it doesn’t work like that.
Denial has never worked for me.
Denial doesn’t kill cancer.
I still believe it could be worse.
I know that is true.
And so, for today, I focus on the fact that I’m not the last one on line.
On the really challenging days sometimes that knowledge is all I have.
And on those days, that knowledge is enough.
October 2nd, 2014 §
 There is comfort in routine.
There is comfort in routine.
Some people are superstitious. Sometimes they want the same chemo nurse, the same appointment time, the same chair. “If it is working don’t mess with it” applies to many things about treating cancer.
I am always thinking about continuity and the stories that objects tell. I’ve written twice about the tape measure my plastic surgeon used to measure me before surgery. I’ll post those pieces again this month.
Whenever I sit in a chair in a doctor’s office I think about all of the people who have sat in that chair before I have.
Each person has a story. So, too, does each chair. That chair is the starting point for this piece from 2011.
………………………….
“I think so too”
That chair you’re sitting in?
I’ve sat in it too.
In waiting rooms. Chemo rooms. Prep rooms. For tests. Surgeries. Procedures. Radiation. Inpatient. Outpatient. Emergency visits. Routine visits. Urgent visits. To see generalists. Specialists. Surgeons. Alone. With friends. With family members. As a new patient. Established patient. Good news. Bad news. I’ve left with new scars. Prescriptions. Appointments. Words of wisdom. Theories. Guesses. Opinions. Statistics. Charts. Plans. Tests. Words of assurance. More bloodwork. Nothing new. Nothing gained. Nothing but a bill.
That feeling you’re having?
I’ve had it too.
Shock. Disbelief. Denial. Grief. Anger. Frustration. Numbness. Sadness. Resignation. Confusion. Consternation. Curiosity. Determination. Dread. Anxiety. Guilt. Regret. Loss. Pain. Emptiness. Embarrassment. Shame. Loneliness.
That day you’re dreading?
I’ve dreaded it too.
The first time you speak the words, “I have cancer.” The first time you hear “Mommy has cancer.” Anniversary day. Chemo day. Surgery day. PET scan day. Decision day. Baldness day. The day the options run out.
Those reactions you’re getting?
I’ve had them too.
Stares. Questions. Pity. Blank looks. Insensitivity. Jaw-dropping comments. Tears. Avoidance.
Those side effects you dread?
I’ve dreaded them too.
Nausea. Vomiting. Pain. Broken bones. Weakened heart. Baldness. Hair loss. Everywhere. Unrelenting runny nose. Fatigue. Depression. Hot flashes. Insomnia. Night sweats. Migraines. Loss of appetite. Loss of libido. Loss of breasts. Phantom pain. Infection. Fluid accumulation. Bone pain. Neuropathy. Numbness. Joint pain. Taste changes. Weight gain. Weight loss. Mouth sores. Fevers. Anemia.
That embarrassment you’re feeling?
I’ve felt it too.
Buying a swimsuit. Getting a tight-fitting shirt stuck on my body in the dressing room. Having a child say “You don’t have any eyebrows, do you?” Asking the grocery line folks to “make the bags light, please.” Wearing a scarf. Day after day. Wondering about wearing a wig because it’s windy outside and it might not stay on. Holding on to the bannister for dear life. Passing out in public.
That fear you’re suppressing?
I’ve squelched it too.
Will this kill me? When? How bad is chemo going to be? How am I going to manage 3 kids and get through it? Will my cancer come back and take me away from my life? Will it make the quality of life I have left so bad I won’t want to be here anymore? Is this pain in my back a recurrence? Do I need to call a doctor? What is worse: the disease or the treatment?
That day you’re yearning for?
I’ve celebrated it too.
“Your counts are good” day. “Your x-ray is clear” day. “Now you can go longer between appointments” day. “See you in a year” day. First-sign-of-hair day. First-day-without-covering-your-head day. First taste of food day. First Monday chemo-isn’t-in-the-calendar day. Expanders-out, implants-in day. First walk-without-being-tired day. First game-of-catch-with-the-kids day. First day out for lunch with friends day. First haircut day. “Hey, I went a whole day without thinking about cancer” day. “Someone asked me how I’m doing, I said ‘fine’ and I meant it” day.
That hope you have?
I have it too:
More research. Easier access. Targeted therapy. Effective treatments. Better quality of life. More options. Longer life. Less toxicity. Fewer guesses.
Ultimately, someday, for my children or grandchildren perhaps: a cure.
Don’t you think that would be amazing?
I think so too.
October 1st, 2014 §
 Today is October 1st. It is officially Breast Cancer Awareness Month. To me every month is Breast Cancer Awareness Month. I will have breast cancer for every minute of the rest of my life. I need no reminder of what this disease is, what it does, what it can do.
Today is October 1st. It is officially Breast Cancer Awareness Month. To me every month is Breast Cancer Awareness Month. I will have breast cancer for every minute of the rest of my life. I need no reminder of what this disease is, what it does, what it can do.
To me, it isn’t about pink products, or a five mile walk, or a bake sale. It’s about life and death. My life and death. It is about having cancer detected early and doing everything possible and still being diagnosed more than five years later with stage IV disease.
October 1, 2012 was the day I found out I had metastatic breast cancer. That was the day my life changed.
The average life expectancy after diagnosis is given as 26 months. Today marks 24 months from my date of diagnosis.
I have a lot to say about October, about research, about education, about how those of us with incurable breast cancer are mostly forgotten. I want to do my part to make the voices of people with metastatic breast cancer heard. I will be posting the link a lot this month to the fund I’ve established at Memorial Sloan-Kettering for research into metastatic breast cancer. This month I will also repost some of my own favorite blogposts and also my most-read pieces. I hope you will find posts you have never seen before and find something new in a post you might have read when I first published it.
Some will be practical advice pieces. Some will be purely poetic. Some will be about me, some will be about our children.
I find that when I re-read a piece I find something different in it because I, the reader, am different. I encourage you to tell me posts that have resonated with you throughout the years that you would like to see again or want others to see.
I’m starting the re-posts today with a piece I wrote only about 6 weeks after my diagnosis of metastatic breast cancer.
……………………………………….
“And Yet the Morning Comes”
Each day is different. Each moment, too.
It still seems surreal, this diagnosis of metastatic breast cancer.
It’s strange how quickly the horrific can become regular: the chemo, the side effects, the new routines.
Oncology appointments, IV infusions, medication refills all start to fill my calendar.
I start making lists of things I need to do. I prioritize them.
It’s not always about what’s actually the most important, it’s also about finding things that bring me small moments of joy.
The small moments are the ones that bring tears to my eyes. Tristan’s little voice saying, “I love you, Mama. You’re the best Mama in the whole wide world” is enough to make me misty.
I still lose my temper. I still yell sometimes. Often it’s misplaced anger, a manifestation of my frustration with my situation.
I haven’t suddenly turned into the world’s most patient person. Sometimes cancer makes me the most impatient one, in fact. I feel the clock is ticking. I don’t have time for nonsense. But that’s not a way to be. I will still try to be better.
I try to be the one to do things with my children as much as I can. Even if there is a babysitter in the house Tristan always reads to me at night for his homework: that is sacred. I still save artwork and photographs and remind them to brush their teeth and clean their rooms.
I try to do the little things: helping Colin with a school project, keeping Paige company while she does homework, watching a sports practice if I can. I go to the grocery store and I work on the holiday card. I still take pleasure in getting the stubborn stain out of Clarke’s dress shirt that the dry cleaner couldn’t.
My motto is that I will do as much as I can for as long as I can.
I don’t ever have a moment that I forget about my cancer. I think that’s the part about it being new. Even when I was diagnosed the first time — even after I finished chemo and surgery and all of it– it still took at least a year for me to be able to push the daily fear down. Of course now the fear has been realized. I am living it. I am living my nightmare, one many people share.
And yet, the morning comes.
I see the light of day and I get out of bed. I see the faces of my children. I kiss my husband goodbye when he leaves for work. Each day I have is a day that matters. Each day is one to make a memory with my family and friends.
Each day is one more than I had the day before.
But let’s be clear: there is no joy in this disease.
My appreciation for my days should not be interpreted as supporting the nonsensical idea that “cancer is a gift.” There is nothing positive about this disease; I would give it back if I could. I did not need cancer to show me the value of things. I always knew these things were true. I never took them for granted. I knew what demons could be lurking.
I did all I could. It was not enough to keep it at bay. But maybe, just maybe, I can keep it at bay for a while.
I still haven’t fully come to terms with what this diagnosis means, but that’s because there’s no real way to know. We don’t know enough yet. It is the uncertainty that is the most difficult part for me. Will this chemo be the one that lasts for a while? Will it fail? When? What next? How long will that one last? My body holds the answers, but it’s not showing its hand yet.
I have to learn to ride this roller coaster. I’m just not there yet. And I don’t really know how long that is going to take.
I walk past people on the street and know they have no idea what is going on inside my body.
People in front of me in line at the gas station don’t know there’s chemo in my purse.
I look like everyone else. I have hair on my head. I ask the checkout person to pack the bags light because I can’t carry anything with my left arm now (the cancer has fractured two ribs on my left side).
Sometimes I want special treatment. I want a Get Out of Jail Free card. Most of the time, however, I want to stay home. Hide out. Be invisible.
I’m still processing. Reeling. But while I’m doing that I’m living.

 The past few weeks have been some of the most challenging this year. By the time you read this I will have had my third Navelbine infusion. Unfortunately, we do not have any evidence so far that it is working. Each chemotherapy that I try at this point only has about a 30% chance of working even for a short period of time.
The past few weeks have been some of the most challenging this year. By the time you read this I will have had my third Navelbine infusion. Unfortunately, we do not have any evidence so far that it is working. Each chemotherapy that I try at this point only has about a 30% chance of working even for a short period of time.










 Link to Twitter
Link to Twitter