January 6th, 2014 §
 The last weeks have not gone as planned.
The last weeks have not gone as planned.
I had the liver biopsy and PleurX drain put in my left lung on 12/31/2013. I was going to only stay one night for observation and to try to address the pain that I was having. Further tests revealed more information. The pain that we thought was coming from my lung and spine wasn’t just coming from my lung and spine. In fact I have some tumors in my bones in the left hemisacrum and right femur too. The spine tumors are now in more vertebrae than we’d thought.
I’ve actually been in the hospital for 6 days now trying to get the pain under control and formulating a treatment plan with my team. I will need to be here for a while longer. I am starting 10 sessions of radiation later tonight after being mapped this morning. We had hoped to do it in five sessions but for reasons I can’t go into now they have decided this is a better route and will be more effective for the future.
This treatment will stop the current progression of pain, but the way this radiation works for me is that it won’t provide true pain resolution for probably about 2 weeks and then improve further over the next few months. The pain reduction will be cumulative and take a while (long after the radiation is actually over) to see final resolution in my case. I’ll have to deal with this for a while yet.
The side effects because of where they are targeting the beams in my spine will be irritated esophagus, trouble swallowing, nausea, vomiting, and heartburn. The other radiation site in my hips will potentially cause decreased blood counts, pain, irritation, gastrointestinal pain and dysfunction and the like.
My pain is still not under control and I’m on a Fentanyl pump system that allows me to dispense medication as needed in accordance with the pain levels. I will convert over to oral medication and patches when it’s time for me to go home once we can figure out my needs. The pain and palliative care team here is unbelievably caring and devoted. So are the physicians and nurses. I have created an expanded family here already and can’t say enough nice things about the quality of care and total commitment to the patient.
I think for now that’s enough news.
Please, please respect my declaration that I do not want uninvited visitors, any gifts, or any flowers sent during this time. I know the intent might be good, but I appreciate so much those who have opted to instead donate to my Sloan Kettering metastatic research fund instead of purchasing anything for me. I haven’t been able to send thank you emails for those recent donations but trust me, they are appreciated. Good thoughts are also always just fine and have the right price tag!
This is a time when I am dealing with severe pain, a medical diagnosis that is unfolding and serious, and needing rest as much as possible. I do read emails but I am not responding to most at this time.
I was not able to start the clinical trial because of these newest announcements. We will see if I am eligible for it again in the future but for now we have to get the disease and pain under control. I did go on chemo for a few days but it now needs to be stopped during radiation. I will resume chemo after radiation is over and about a week of recovery time has elapsed.
Things change hour by hour, day by day. I’m adjusting the best I can. I hope this will at least let you know where we are, a long way from where I thought I’d be in the first days of this new year. Welcome to the world of metastatic breast cancer.
October 1st, 2013 §
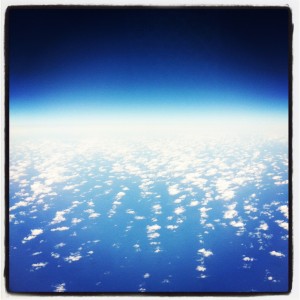
 This is the last photo I took before I found out I have metastatic breast cancer.
This is the last photo I took before I found out I have metastatic breast cancer.
This photo was taken in the final days of September when I went to visit my surgical oncologist for my annual checkup.
I’m wearing a hospital gown with those boots. The contrast of the gown and boots made me laugh.
I snapped the photo.
The actual diagnosis came one year ago today.
It came on the first day of Breast Cancer Awareness Month (a month which has always driven me batty).
It came more than five years after I finished treatment for stage II breast cancer (no, five years without a recurrence does not mean you’re cured, let’s just bust that myth right now. Hormone receptor positive breast cancer in particular can return after 5, 10, 15 years or more).
……
I went to my surgical oncologist annually so she could check on how I was doing after she surgically removed both breasts in January of 2007. After the active post-surgery period, the visits consisted mainly of a physical exam and a talk about how I was doing and what post-chemo treatments I was on.
At this particular visit I complained of some rib pain in a place where I’d broken two ribs in a fall a few years prior. Nothing else was bothering me that day. While I was changing into my street clothes she phoned downstairs to my medical oncologist who said he would put orders in to repeat my bloodwork a month early. It was a test he did every six months at that point.
None of us were worried.
Flash forward a few days to Monday, October 1, 2012.
One of my medical oncologists (I have two, one is a general hematologist/oncologist and one is a breast oncologist) walks into the room with a concerned look on his face and says hello and goes straight to the computer. He starts punching things in to log into the system.
I ask him, “How are you?” “Not so good,” he says. I am sure he’s talking about himself, his family, his favorite sports team perhaps.
“Your markers are elevated,” he says. And only then does he turn to make eye contact with me. I know now, looking back on it, it was too hard from him to tell me. He really didn’t want to deliver that news that day.
When he tells me, he knows I know what that means. We’ve been a team for more than five years by then. He knows I know. It doesn’t need to be explained.
He looks at me while I crumble. And swear. A lot. He comes over to comfort me. I am alone in that room with him. No one expected this to be anything but routine. I didn’t bring anyone with me for the appointment, I almost never had company with me at any of my appointments over the years. That’s how I liked it most of the time. I still do, actually.
But today’s visit rapidly becomes the farthest thing from routine.
……
I wasn’t expecting it. I confess that. The pain I’d complained about a few times during those five years? That pain had never turned out to be anything.
And oh… by the way, that rib pain that I complained about? It actually was nothing. It was just sore ribs from the old fractures.
I was sent across the street to the hospital immediately for a chest x-ray. This looked clear. My PET scan the next day showed no cancer where I’d complained of soreness. But there was cancer elsewhere: in multiple bones and lymph nodes. It really was what we feared. We were lost, falling, reeling, grieving.
Within three days I was having a surgical biopsy through my neck to gather malignant tissue and lymph nodes. Within two weeks of the news I had the true sign that would have taken me to a doctor anyway: bone pain in my collarbone area from a fractured first rib caused by cancer breaking through the marrow into the bone.
I’d have found out within a few weeks that I had metastatic cancer anyway when the pain in my shoulder got severe… which is why some doctors don’t even use tumor marker tests. The marker tests don’t reflect cancer activity for everyone. Physical symptoms are usually quite reliable. And let me also point out that a lot of muscular pain can be hard to distinguish from bone pain depending on location. I’ve had both. And it’s not easy to tell them apart in my opinion.
I went and met with my other oncologist a few days after that.
I started chemo within ten days of hearing my diagnosis.
Things moved fast.
Life changed forever.
……
The weather is changing now. It’s warm this week so I don’t think I’ll be reaching for those boots.
But when the cool air comes again in a week or two or more I am not sure how I will feel when I reach for them.
Right now they just make me feel sick.
September 23rd, 2013 §
 It takes a leap of faith every day.
It takes a leap of faith every day.
Not one of religion– no that’s not in my play book.
But there is a leap that comes when you think to yourself each night,
“The world will be here tomorrow, and I in it.”
Statistically it is likely to be so.
But what about the day after, and the day after that?
How many days do you think ahead?
Have you bought plane tickets for next year?
Planted bulbs for Spring?
Bought an extended warranty on the washing machine?
Three years ago, without even a thought, I took a three year car lease.
Nine months later I received my diagnosis of metastatic breast cancer.
Fifteen months from now that lease will come due.
Will I take another?
I have a car in mind I would love to have…
But can I think of my life in fifteen months,
What it will be,
What will I be?
No, I cannot.
I talk of taking trips in Spring. I have a friend down South I want to visit.
I do believe I will be alive.
But what will my quality of life be?
What chemo or radiation or surgeries will I need by then?
What regimen will I be on and how will I feel from it?
Just being alive is not always enough.
I don’t buy those tickets,
But I do still think the thoughts.
I don’t make promises because I don’t want to cancel.
I say, “Let’s play it by ear,”
“Let’s see how it goes,”
Because to plan, to get hopes up,
To think it could come true…
And then to have them dashed
Would be too hard for me.
I know not everyone shares this view.
The thing with incurable cancer is I don’t have a particular kind of hope anymore:
I can’t have the confidence the suffering will end because it is temporary.
It is not temporary.
I do keep pressing forward though, in my own way:
With strength, with dignity, and yes, still with great hope for more time.
Many days that is one of the hardest things about it all:
I can’t just mark the time and get through
Knowing the hardest parts will soon be over.
Because I know the hardest parts are yet to come.
April 28th, 2013 §
 It is easy to be happy when you are healthy.
It is easy to be happy when you are healthy.
It is harder to know that this may not be true much longer.
People love to casually say,
“Enjoy every moment” or
“We all die some day anyway” or
“Life is fleeting.”
I know this already.
And I know it in a different way.
I don’t need to be told to
fight the good fight to beat it
or the key is to just stay strong
or that it’s mind over matter
or that I should pray for a miracle
or that I will be cured.
That’s nonsense.
Scientifically impossible in my case.
And so, when you say,
“No, that can’t be true.
There must be something that will cure you,
If you want it/pray for it/think it will be so,
You can be healed,”
What you do is force me to assert my knowledge,
Insist upon my diagnosis,
Explain the desperate nature of my disease,
Spend my time defending my sentence.
I know it’s what you wish.
I know you insist because you want it to be the case.
I know you’re grasping at straws,
Wanting to reassure yourself that bad things won’t happen to you,
That bad things don’t happen to good people,
That something awful won’t happen to me.
Trust me, I wish for it too.
But these things do happen.
It has happened to me.
The truth is that wishes don’t count for anything when you’re placing them against cell biology.
I know many healthy people who say the passage of time is bittersweet.
It isn’t a competition but I can tell you that this passage of time is different.
If you could feel it for just a moment you would know.
There is a difference between
Distant,
Hypothetical,
Potential,
Maybe…
and reality.
I have learned that being nervous about test results,
Worrying,
Wondering,
are not the same as the reality.
Reality is having your oncologist walk in the room
and when you say to him, “How are you?”
and he says, “Not good,”
you naïvely think it must be a problem with him,
or his family and
instead he ducks his head,
takes a breath,
looks at you, and says,
“Your test results were not good.
Your tumor markers are up.”
He knows I know what this means.
He waits for a moment and says,
“I think you have a metastasis.”
A few minutes later he says,
“You need to go get a chest x-ray right now.
Go across the street,
I will come over to the hospital and look at it immediately.
Wait for me there.
Then you need to schedule a PET scan as soon as possible.
Have you had any other unusual pain?
A cough perhaps?”
The room spins, the world stops.
My life didn’t end in that moment, but life as I knew it ended for sure.
No turning back.
Reeling, processing, shock.
All you can do is let your jaw drop,
the tears fall,
your body shake,
crumple.
Slowly,
deliberately,
as I looked at him
in a way that I never had in the six years he had been my doctor,
the only words that came to my lips in response
were to repeat over
and
over
and
over
and
over
again:
“Fuck. Fuck. Fuck. Fuck.”
Because that’s the only word that could capture how angry
and scared
and angry
and surprised
and angry
and shocked
and angry
I was.
I never have liked the term “to expire” rather than “to die.”
I started thinking about these words though.
We all have an expiration date.
I’ve never thought of it like that before.
We all have one.
It is as if I’ve grabbed a carton of milk without looking.
I took the one in front I guess,
The one with the rapidly approaching date they put conveniently at the shelf’s edge for people to grab when they’re not paying attention.
Except I did pay attention.
I did.
I was always paying attention.
No one was more vigilant than I.
I want to put this carton back,
I want to say it’s not mine.
I want to scream it.
This must be for someone else.
The date is too soon but I can’t trade it in for a new one.
No givebacks.
The problem is
I don’t know exactly what the date says.
April 12th, 2013 §
I want to just send out a quick clarification about my chemo because I can tell from messages I’m getting that I didn’t explain well what has happened with my discontinuation of Xeloda. This particular chemo is now failing, yes. But that doesn’t mean it didn’t work. This is part of this disease of metastatic breast cancer. In some cases the treatment option never works; that is, your cancer doesn’t respond at all. You get no benefit from day one. You abandon it quickly.
Mine, however, falls into the other camp: it did work for a period of time. It did what it was supposed to, just for not as long as we’d hoped. That is, it did reduce the amount of cancer in my body for a while, it did hold progression at bay.
It’s no longer doing that, my counts are very slowly rising, but that doesn’t mean it “didn’t work.” It just means it didn’t work for as long as I would have liked.
Most people with advanced disease will be leapfrogging around all sorts of agents (chemo, anti-hormonals, etc.) to try to see what works. The cancer mutates and becomes resistant to most treatments that will get used. That’s when it’s time to move on to a different one. I know people that have been on at least ten different agents. That leapfrogging is just the nature of the path many others and I are on. A small percentage find one that works and it continues to work for a long, long time. Research is needed to find out why these particular cancers are more easily tamed. We do not know now why that is the case but researchers are learning more and more about the subtypes.
So while the stability was not as long as we’d liked, in this particular case it doesn’t mean it didn’t work. It did. For six months. But now we’re moving on.
In my case, because my cancer is estrogen-receptor positive, we’re trying anti-hormonal agents. Although I don’t have ovaries to produce estrogen, the fat cells and adrenal glands in my body still produce estrogen. I will be taking two drugs every day now, Aromasin and Afinitor. The plan is in place and I’m already starting taking them, slowly on the Afinitor because it has a side effect of bad mouth sores if started at a full dose. I won’t go into other side effects here because I don’t know yet what my particular response will be.
Thanks for all of the notes of support and concern over the last 48 hours during the PET scan and this new adjustment. As always, I can’t respond to every message but I do appreciate them all.
January 31st, 2013 §
I always think these updates must be boring to read. I know they’re necessary, and important. I know this is how most of you get the nitty gritty details on my treatment. Somehow, though, I always wonder if they are actually educational or if they are too technical. So, that’s why I try to limit them to about once a week or when there are changes. My goal is to show you how these decisions get made (in my case only). Some cancers have very specific and formulaic treatment schedules. Metastatic disease often does not. It’s unclear which drug(s) will work and for how long. It’s never known how a patient will tolerate the drug initially and cumulatively as time goes on. The patient has a lot of leeway in many of these cases. There is no blueprint. A good team has communication about options and constantly revises their strategy.
I had this week “off” from chemo. The last few days I’ve felt very good. I have been spending lots of time with our new dog, Lucy, who has brought joy into our home in so many ways. We just adore her.
I was at Sloan Kettering last week and today I met with my local oncologist. Fortunately everyone in agreement after a review of all of the options. One of the things that’s always a concern is quality of life. My doctors are very keen on making sure I am comfortable and able to do things I enjoy. The balancing act of aggressive treatment to extend life without sacrificing too much quality of life is an integral part of treating metastatic cancer. There is no cure. But the goal is holding off the inevitable as long as possible.
I’ve had lingering trouble with the monthly IV bone drug Zometa. Some readers suggested I ask about the other available drug Xgeva, a subcutaneous injection also given once a month. They anecdotally reported fewer side effects. Both of my doctors do not believe Xgeva actually is better for my needs cancer-wise than Zometa, but also agree it’s not worse. One option was to try an IV steroid infusion of Decadron immediately prior to the Zometa to see if it helped with side effects. The other option was to try to the Xgeva and see if I had any side effects from that (most people report fewer to no problems with it, though most also do not have problems with Zometa after the first one or two times). I’ve opted to try the Xgeva. I would usually have gotten it today (28 day interval) but I have plans this weekend that are very important to me. I don’t want to risk being ill and having to cancel. It will not be a problem to get the injection on Monday, so I will postpone it for a few days. We’ll see how I tolerate the Xgeva shot and go from there.
My tumor marker number stayed relatively constant after that small increase two weeks ago. This is good, but leaves us in a bit of a quandary. We aren’t yet at the point of doing a repeat PET scan. The rise is not enough to warrant that, though we will do it soon. Neither is the increase enough to assume the chemo has stopped working after initially being responsive. We don’t know, as I said in the last update, if it’s an anomaly or a trend. The only things that can show us are more data points. I happen to like data points. I like seeing what happens every 2 weeks even if it means more of an emotional rollercoaster. We are only 4 months into this and I don’t feel that we have a handle on how I’m responding yet. Only time can shed light on that. I did have a good initial reaction to the drug which was encouraging.
So… since we’ve achieved a good decrease in the last 4 months with the Xeloda but now that is slowing down and I seem to have “bottomed out” on its efficacy, what now? We want to keep everything where it is. If we can get more of a decrease, that’s the best. If not, we need it to hold steady. We all agree it’s time to try again to increase the chemotherapy dose and see if I can both tolerate it and get a stronger marker response. I started at 8 pills a day in the beginning (for about 2 months) and had to decrease about two months ago to 7 pills a day when side effects became intolerable.
It’s time to walk into the fire again. There is no manual for how to do this. We all brainstorm, we talk about what my goals are, we talk about what makes scientific sense. The idea this time is to increase, but not go back to the 8 pills for the whole round. Instead, to try to get more chemo in my system, I will alternate 7 and 8 pills for the week. We’ll see how I do. Debilitating nausea, stomach pain, hand/foot syndrome, and migraines have been my issues with this drug in the last month.
Also, I will change my start day. Thursday night was my usual. Lately, however, I’ve felt rotten on the weekends (both weekends this time around, as effects often last into day 10 or 11 which technically are “off” days for me). I will now start chemo on Saturday night or Sunday morning and see if we can shift my “rotten days” to weekdays instead. I want more quality days with my family on weekends if I can get it.
This is all educated guesswork, a constant dance of drugs and schedules and side effects and efficacy.
There is no manual.
There is no “must.”
There is only me, floating away, trying to grasp the fingertips of treatment and hope.
January 9th, 2013 §
Elizabeth Edwards reached many people because she was in the public eye, but inspirational people also live quiet lives. We can be inspired by Edwards’s grace and courage as she dealt with the challenging parts of her life in the same way we can find inspirational people around us each and every day. These are all people we can connect with and learn from. In doing so, we better ourselves.
When she was diagnosed with metastatic cancer people told me not to worry: it wouldn’t happen to me just because it happened to her. That’s true. It wouldn’t happen just because it happened to her. But it did happen. And now I look back on everything I’ve said for the past 5.5 years and I am glad I expressed those thoughts as they were happening. Because my fear came true.
…………………………………..
(from December 7, 2010).
I didn’t know Elizabeth Edwards. In fact, I wrote a piece critical of her when she initially stood by John after his affair. I was disappointed when she gave an interview on CNN in May of 2009 and spoke only of John’s “imperfection” rather than calling him the cheater he was and kicking him to the curb. I was angry she hadn’t used her interview time to talk about herself, her cancer, her life: the topics I wanted to hear about. I was angry at her for not claiming her remaining years of life as her own.
So why am I sitting with tears in my eyes because she has died?
I cry because it makes me feel vulnerable and scared of what this disease can do to me: what it did to her.
Yes, I know… there are plenty of men and women who get cancer, have treatment, and stay in remission for the rest of their lives. And, in essence, isn’t that what every cancer patient hopes for, as Betty Rollins wrote, “to die of something else”?
I don’t think it makes me pessimistic, depressing, or negative to think that I am vulnerable.
It’s the truth. It’s my truth.
Anyone who hasn’t been to the oncologist with me to see my risk-of-recurrence charts, my mortality charts, my decision-making discussions along the way can’t say to me “Oh, don’t worry, that won’t be you.” No one, including me, knows how it will go.
People tell me: stay strong, just think positive, you can’t generalize from her situation.
I respond: I am strong, I hope for the best. I don’t think positive thinking is going to save me if there are remaining cancer cells still in me.
I hope that people won’t say to someone who has been diagnosed with cancer, “Don’t worry, what happened to Elizabeth Edwards won’t happen to you.” Because while we do everything we can to ensure we die of something else, it just isn’t always the case. In 2006 her oncologist told her that there were many things going on in her life, “but cancer was not one of them.” Things change quickly, cancer can recur when you least expect it.
I have sympathy for her family. I cry for her children. I am saddened about the years she spent with a man who didn’t deserve her. I am angry about the time she wasted on him. I hoped she would be an example of someone who would keep cancer at bay.
I grieve for that hope, now gone.
December 8th, 2012 §
I realized it’s time for an update… but confess I’ve started and stopped this one a few times. Somehow when things are going along somewhat easily it’s easy to do the updates.This is the first one I’ve had to discuss side effects and I hesitated a lot about what to write and whether to post it. I wasn’t sure about talking about these things lest they be seen as complaining. My goal has always been to educate and inform above all.
Friends on Twitter assured me that talking about the daily in and out of chemo treatment for metastatic cancer is important. Not only are they learning what it’s like, but it tells people what I’m dealing with and what activities might be hard for me on a daily basis. One Twitter follower also said that for those who have family members with this disease and might not be forthcoming with detailed information, some of these updates give them an idea of what it might be like for their loved ones. While treatments and surgeries vary so much, I thought this was an excellent point.
I also have decided to post this information because I know other metastatic patients will find it through search engines and maybe it will help them. So… I’ve opted to continue to share these things. It’s the reality of cancer. It’s the reality of MY cancer.
I’m struggling at the moment with Palmar/Plantar Erythrodysesthesia or Hand/Foot Syndrome (HFS). This is a common side effect of Xeloda, the chemo I am currently taking. In short, the capillaries in the hands and feet rupture and the chemotherapy spills into the extremities. Redness, swelling, burning, peeling, tenderness, numbness and tingling can accompany it. While it does not always start right away, once you’ve had a few rounds it’s likely to be a cumulative effect.
After receiving another monthly IV infusion of Zometa to strengthen my bones on Tuesday, I started a new round (#5 for those of you keeping track at home) on Thursday night, and had to decrease my dose slightly to deal with the HFS. Rather than 8 pills a day (4000 mg) I’m on 7 now. The hope is that the HFS will stay at its current level and not progress on this dose. This is what feet start to look like with HFS:

It can get much worse than this with blisters and ulcerations but mine is not at that stage. If it were to reach that point we’d have to stop chemo until it healed and then re-introduce it. Driving was one of the hardest things yesterday, the pressure from the steering wheel (or anything against my hands) was difficult to tolerate. I wear cushiony gloves most of the day now and follow all of the guidelines to keep it at a minimum. My hands are more sore and sensitive than my feet this week but not as red as my feet. Thankfully while I could not hold a pen during most of the day, I could still do some typing. A long-term side effect of this particular drug is the potential to lose your fingerprints. I see an episode of CSI coming on that one! An article about the difficulty traveling with such a condition appears here.
Loss of appetite continues to be an issue but my weight has stabilized after a 20 pound loss in the first 6 weeks. It’s weight I needed to take off anyway, actually. I must eat twice a day when I take chemo and once I start eating I usually do just fine. I do better eating in the evening. My blood counts remained fine even during the weight loss and my instructions have been to “keep doing what I’m doing.” The one thing I can’t do is exercise at the moment. Friction on my feet can exacerbate the HFS so for now it’s not happening. A soon as the rib in my shoulder heals I will be trying to get back to Pilates class.
I’ll be back at Sloan Kettering on Tuesday, 12/11 to meet with my oncologist. We’ll evaluate the HFS by then and talk about ways to help me deal with it and make me more comfortable. We will also then be talking about what dose I will take for my next round and also start talking about when my next PET scan will be.
That’s the update for now, I’m still doing everything I can and am out and about as much as possible. I still bring the kids to the bus in the morning and try to do errands like the grocery shopping as often as I can. I ask for help with things that really are tough on my hands like stuffing the holiday cards or doing laundry or dishes. Even small tasks give me a sense of accomplishment and normalcy so while the weather holds I continue to do them. Once ice and snow set in and my concerns about slips and falls and bone breakage rise I will get help with more of the outdoor things.
I’ll have more pieces coming out on HuffPo shortly; thank you all for the excitement and congratulations about that new venue. My piece about what to do as soon as you are diagnosed, especially in regard to children, will be the next one they post. After that I’m looking at writing on the topics of bravery/inspiration, the situation when people you barely know take your condition as seriously as if they were family members, and the story of how I found out I had metastatic cancer to begin with. If you have any topics you’d like to see a piece about leave a comment or email me via the contact form and I’ll definitely take it into consideration!
Thanks for all of the support this week.

 The last weeks have not gone as planned.
The last weeks have not gone as planned.


 Link to Twitter
Link to Twitter