November 27th, 2013 §
 Next week I am meeting with a group of oncology Fellows at Sloan-Kettering to talk about care of the metastatic breast cancer patient. I have many ideas of how I think patients and doctors can better be “partners in care.” I have thoughts about how patients can be better in their interactions but this particular session focuses on the physician side of it.
Next week I am meeting with a group of oncology Fellows at Sloan-Kettering to talk about care of the metastatic breast cancer patient. I have many ideas of how I think patients and doctors can better be “partners in care.” I have thoughts about how patients can be better in their interactions but this particular session focuses on the physician side of it.
I will spend my time there emphasizing the things doctors can do in their future careers that will be most appreciated by their metastatic breast cancer patients. Having a supportive, educational partnership is essential.
I have pages and pages written on what I think makes a good oncologist but am not writing about them here yet. I really want to use today’s post as a forum to let you have input. Patients vary in what they want from their doctors. There isn’t necessarily a formula that will work every time. This is part of the message. It is important to find the right chemistry between a doctor and patient especially when you know this relationship will probably be taking you until the end of your life. Some oncologists start to distance themselves from their patients when they know they can no longer “fix” them. I am fortunate that mine are supportive. The balance between quality of life and quantity of it instantly becomes the metric after a diagnosis of incurable cancer. Everything is filtered through this lens.
I encourage you to comment on the post rather than email me. Even if you comment as Anonymous or with initials or even using your diagnosis as your name… I think reading what others think is important for this one. If you feel comfortable doing so, please indicate whether you have metastatic cancer.
So, without sharing my suggestions I’m asking for your input. Feel free to use these questions as jumping off points. Answer one, answer more that one, suggest something I haven’t even brought up.
I am interested in hearing from you what you think about some of the following topics and please be as specific as possible:
What is your preferred method of delivery of test results (ranging from the initial diagnosis to routine followup bloodwork and scans and biopsies)? Some results are given when only the patient is present. How do you feel about that? If you are called and told to “bring someone with you” you would that make you even more upset? In regards to bloodwork, scans, biopsies: do you always want those results in person even if it means waiting longer for those results? Do you mind if the results are by phone if that gets you answers quicker? Do you want the doctor to “cut to the chase” or do you feel more comfortable with small talk first?
How do you want a doctor to respond if you get emotional when you hear bad news?
Do you mind if your doctor gets emotional when delivering bad news or discussing your treatment? Does that make you more upset/scared or do you think that shows compassion?
A new report showed that patients don’t like when doctors talk about their own situations to try to show compassion (“self-disclosure to show empathy”). How do you feel about doctors sharing their personal stories of their own cancer or medical conditions, that of their family members?
Do you like when a doctor admits that he/she isn’t sure which treatment option is best for you or does that bother you?
Do you like when your oncologist presents the one treatment option he/she thinks is best or do you like your oncologist to present a few choices and then you decide together?
Do you like when your doctor asks you questions about your personal life/family/interests? Does your doctor do this regularly?
Does your oncologist talk about your prognosis and if so, what are ways you prefer those discussions to happen?
Do you want a doctor to give you a life expectancy prognosis even though we know those estimates are right only about 20% of the time? Do you want them to discuss it only if you bring it up? Do you like to hear statistics about treatment success and odds of survival?
How much monitoring do you like? Does your doctor give you a choice in how often to conduct tests? Do you feel that tests get in the way of living the life you have left or do you need the results to know where you stand in your treatment?
What is the best way a doctor has communicated bad news to you? The worst? (having a few examples of what not to do can be instructive here)
In the metastatic community in particular there seems to be so much of a focus on treatment and the nitty gritty of all that’s demanded to just treat the disease week to week, month to month. That is only one part of managing it. Have you been offered counseling for services like mental health? Palliative care? Family services? Physical therapy? End of life counseling? Would you like those to be offered to you?
How important are things like scheduling, having phone calls returned, having ways to contact your physician/office that are reliable, even after-hours?
If your doctor asked you to fill out a questionnaire with some of these questions on it would you find that impersonal or an attempt to learn more about you and how to best help you?
Would you like your doctor to have printed material with general definitions of terms and words important to your care (drugs, procedures, tests)?
Would you like them to discuss support groups? Have you asked? Have you been told there isn’t one for your kind/stage of cancer?
And finally: If you could give young oncologists one piece of advice, what would it be?
…………………………….
Thank you for your input. My advice on these topics could probably fill a book. I have a feeling yours could, too. I will try to address some of these topics in future posts.
By the way, I may not be posting over the next few days because of the Thanksgiving holiday.
As always, thank you for your daily support here, on Facebook and on Twitter.
November 26th, 2013 §
 On Friday morning after I sent our three children off to school I traveled to Memorial Sloan-Kettering Cancer Center (MSK) to have a port implanted. My first appointment of the day was at 10:15 to have an electrocardiogram (EKG/ECG). MSK requires an EKG on one of their machines within 48 hours of the port procedure. It takes longer to find the bathroom than it does to have this test done. Electronic leads are attached with sticky sensors to specific points all over your body and hooked up to a machine. After about one minute of recording you are done, and the sticky round patches and the attached wires are removed. Easy as can be. The test measures the electrical activity of your heart to make sure it is normal. I won’t go into details on this test because it’s such a piece of cake and so common.
On Friday morning after I sent our three children off to school I traveled to Memorial Sloan-Kettering Cancer Center (MSK) to have a port implanted. My first appointment of the day was at 10:15 to have an electrocardiogram (EKG/ECG). MSK requires an EKG on one of their machines within 48 hours of the port procedure. It takes longer to find the bathroom than it does to have this test done. Electronic leads are attached with sticky sensors to specific points all over your body and hooked up to a machine. After about one minute of recording you are done, and the sticky round patches and the attached wires are removed. Easy as can be. The test measures the electrical activity of your heart to make sure it is normal. I won’t go into details on this test because it’s such a piece of cake and so common.
After that test was complete (by 10:08) I went to a different floor in the same building to the Interventional Radiology department. There, a friendly team checked me in and sent me to the waiting room, a large attractive area brimming with patients and family members. After a little while a woman called my name and I was taken back to be prepped for surgery about 30 minutes before my scheduled 11:15 arrival time. I will say that for every test and procedure I’ve had so far at MSK’s main hospital they have been on early or on time. This has been a pleasant surprise at such a large medical center.
Once we reached a small prep room a very cheerful nurse gave me a garment bag to store my clothes in and I changed into a standard issue hospital gown with a thin navy blue bathrobe to wear over the top. She weighed me, measured my height, and reviewed my medical history. This was the first surgery I had at MSK so I had to review my surgeries and allergies along with current medications, etc. They wanted to do another pregnancy test but I refused on the grounds that I had an oophorectomy and the test was unnecessary. Because the surgery had not been done there they didn’t have the exemption in my file. They confirmed that I had not used any blood thinners (including medications or pain remedies that can act as blood thinners) in the days prior to surgery.
I then met the surgeon for the first time and he and I discussed the precise placement site of the port and also the ramifications of my sensitivity to adhesives. Usually it’s not too much of an issue but for this procedure the surgeons usually close the incisions with Dermabond (skin glue) and my skin cannot tolerate that. Sutures would be used instead.
The surgeon pinched the skin between my collarbone and the top of my breast implant and said that there was enough tissue there to use the preferred port, called a MediPort or PowerPort. Each person has a different amount of fatty tissue in this area, and a mastectomy may affect this as well. Age, body type and other factors can affect which model of port can be used and where it will be positioned. Obviously, children and people using a port for only a short period of time may have different limitations and needs. There were a few times during the day when someone said to me, “You’ll just have this for a while and won’t even know it’s been there after it’s gone.” They assumed that I would only need it temporarily. “It’s here for good,” I said more than once.
There are many different kinds of ports. They have changed a lot over the years. The one I have is quite small and is triangular in shape. This shape is an indicator that the port can be used for injections of contrast dye (these are called “power-injectable”) in addition to being used for blood draws and any future IV chemo. The power-injectable feature means that when I go for CT scans, bone scans, or PET scans, the technician can inject any dye that might be needed for that test into the port rather than having to use an IV line into my hand or arm. This is one reason I decided to get the port. Being in clinical trials now means frequent blood draws and scans.
The nurse started an IV in the holding area and I was wheeled through a maze of hallways until we stopped outside the operating room. I got off the gurney, walked into the OR, and hopped onto the table. After a lot of prep including hooking me up to monitors and draping and cleaning the area, they finally pushed Fentanyl and Versed into my IV. I didn’t actually go to sleep but probably could have. They numbed the two incision areas with local anesthetic and after about 15 minutes including a few periods of tugging and pushing it was over. I’m going to just link to the actual description that MSK gives about the procedure itself. I’m not sure I can explain it any better than they do.
I stayed in the OR for about ten minutes and then was wheeled to a very small private recovery room where I stayed for about an hour. The one surprise is that in the Interventional Radiology department’s recovery area at MSK they do not give you anything to eat or drink after procedures. So I needed to wait until I left to have anything (tip: if you are going to have a port placed, tuck a snack and drink in your bag. After fasting until the procedure you will want something convenient to eat and drink afterwards and radiology departments might not provide them the way that surgical recovery areas often do).
My husband was able to join me in this recovery area after I was settled. A nurse reviewed my discharge instructions. I needed to wait slightly longer to get the incisions wet than usual because I did not have the Dermabond. Usually it’s a 1-2 day wait. I was quite sore immediately after and was glad I had put a cushion and pillow in the car. If your port is put on the right side, as mine is, the passenger side seat belt will not be pleasant so I recommend bringing a padded seatbelt cover or other method of cushioning the strap. I was quite sore for about 24 hours, but quickly that shifted from being generally aware of the pain to being very localized and only when using that arm. That quickly became localized discomfort if touching it. Today (three days later) it’s still sore to the touch but otherwise not bothersome. I did not use any pain medication.
The port is much smaller than I would have thought. It’s placed so low that it won’t be visible in a tank top. The surgeon was very careful to try to pinpoint a location that would be cosmetically most appealing which I appreciated since this will not be temporary. Eventually I will need IV chemo and this will be used for that as well. For now there are two red incisions but I know those will fade. They are far more visible than the port, a bump under the skin the size of a quarter.
I will not be able to use the port for blood draws that I do near my home and many people are not aware that not all phlebotomists can access the port. Only certain people (most often at hospitals and oncology offices) can access the port because you need special training and also special equipment. In addition, if you do not use the port for a period of about 30 days you must go to have it flushed (with saline and Heparin) to prevent clotting. It only takes a minute to do that.
I’m happy to answer any questions that readers have about the port or anything I missed in the description.
…………………………………
Today I was back at MSK for my regular clinic day for Cycle 2, Day 1 of my clinical trial of Genentech GDC-0032 + Faslodex. I met with a nurse first who checked my weight, blood pressure, oxygen saturation, did a physical exam, reviewed my side effects (I won’t go into those in this post). Next I met with the Principal Investigator on the trial who is the one in charge of my care during this time. I gave her the four remaining pills of my 30 day supply (two each of 1 mg and 5 mg capsules of GDC-0032) and signed and turned in my medication log which lists what time I stop eating each night and what time I take my pills each morning. We discussed scheduling for the month which includes my CT scan three weeks from now where we will get our first look at what, if any, effect the drug combination is having on the cancer.
Next I went to the chemo suite to get my Faslodex injections and have my blood drawn as required by the protocol. I had a different nurse this time from the last two times. I told her that I had a new port and asked her to explain the process for the draw now. She warned me it might be sore as she palpated it to find the right spot to insert the needle and also said the actual needle stick might be a bit more painful today depending on the exact location of my incision.
We each needed to put masks on to cover our nose and mouth during the blood draw to minimize the chance of infection. She gently felt for the circular center of the port where the reservoir is and inserted a special needle to access it. It was a bit tender but certainly not at all more painful than my usual stick on the back of my hand. It really was just a second and it was great to know there was no chance of “failure”… blood would flow! And it did. Six tubes were done quickly and then she flushed the port with saline and Heparin to prevent clotting. The needle was removed, a gauze and paper tape bandage applied (no adhesives for me) and then we removed our masks. Easy and no anxiety. These steps must be taken every time.
Next it was time for the two nasty Faslodex injections. As I’ve written before these are two jumbo intramuscular injections, one in each butt cheek. The nurse kept apologizing and saying how she hates to give them because they’re just so big and painful. They are always very sympathetic when administering these. Today’s were painful, I think the worst of the 3 rounds I’ve had. I think it’s just chance about where they hit and also that I’ve had to do them every two weeks this month during the loading phase. Now I will only need them every month so there is longer recovery in between from the soreness and muscle pain. I find that a heating pad is the most comforting way to ease the pain, I’m definitely getting used to it and also knowing what to expect.
Once done I stopped into the pharmacy (right next to the chemo suite) to pick up my next month’s supply of GDC-0032. I needed to wait to take today’s dose until after my bloodwork. I took my pills with a glass of water while still standing in the pharmacy and noted the time in my new medication log. I would now need to wait one hour before eating or drinking (as I always do when I take my dose each morning).
I went down one floor to scheduling, made my next appointments, and was on my way about 2.5 hours after I first walked back to the exam room. I met a friend for breakfast and had that blissful first cup of coffee at precisely the time allowed. I took the train home, and fell asleep on the way.
I’ll be back at MSK in two weeks for an appointment with the doctor and bloodwork. The week after that will be my scan and then I’ll be back again a few days before Christmas to begin Cycle 3 if all is stable.
If my cancer has grown (“progressed”) by 20% or more, however, the drug combination is deemed not working. I will stop the trial (and be dropped from it) and I will need to move on to something else. I’m already at work researching what that next choice should be.
…………………………………….
We are entering a fragile time of year. The holidays are difficult for many people. Some miss loved ones who have died. Some mourn their own lives, no longer what they were. Grief takes many forms. The pressure to create memorable and uplifting occasions can sometimes be oppressive.
Be kind to those who are struggling during this time; physical and mental illnesses can be especially difficult to manage. Understand that happiness and sadness can coexist. Reach out to others if you can.
Find a bit of beauty in the world. Share it. If you can’t find it, create it. Some days this may be hard to do. Persevere.
November 24th, 2013 §
 I could not have known at that time the path my life would take. I could not have known how my words were reaching into the future, knowingly, achingly.
I could not have known at that time the path my life would take. I could not have known how my words were reaching into the future, knowingly, achingly.
I originally wrote about Katie Rosman’s book If You Knew Suzy in 2010. The blogpost was written before my diagnosis with metastatic breast cancer but years after my diagnosis of stage II breast cancer. My fears, articulated below, of my cancer returning and taking me from my family have now come true. It is interesting to read my words now through this new life lens.
Katie and I have grown so close since I first wrote about her book, her mother, and their effect on me. Our friendship runs deep. I treasure Katie’s thoughtfulness, her compassion, her devotion to her family, her laugh, and yes, I’ll say it: I am very jealous of her curly hair and ability to do handstands.
………………………..
November is Lung Cancer Awareness Month. Misinformation and stigma are still linked with lung cancer.
I get asked all the time, “Why do you think you got cancer so young the first time? Why do you think it metastasized?” I think people are searching desperately for identifiable reasons so they can feel “safe” from the fate I have (Clearly she must have done something to be seeing it once again, right? That won’t happen to me, right? If I just eat this or drink that it won’t happen to me, right?).
There is one question almost universally asked of those diagnosed with lung cancer: “Smoker?” There are many risk factors for lung cancer that have nothing to do with smoking. In fact, I only learned after having an oophorectomy in 2008 that surgically-induced menopause significantly increases the risk of lung cancer (one paper here).
Yes, current smokers are those most likely to be diagnosed with lung cancer. But there are increasing diagnoses of those who have never smoked and many who stopped decades ago. We need much more research into the spectrum of causes of lung cancer (including radon and asbestos exposure) and effective treatments. The stigma associated with it, however, is a barrier to raising money for research compared with other cancers. It is the deadliest cancer; more than 25% of cancer deaths are from lung cancer (more than from colon, breast, and prostate cancer combined) yet receives only a fraction of research funding.
I wanted to share this post again during Lung Cancer Awareness Month to highlight one life. Writing is powerful. Across time and space, without ever having heard each other’s voices or shaken each other’s hand, I have learned so much from Suzy.
Katie’s mother, Suzy Rosin, died from lung cancer.
……………………….
There comes a point in your life when you realize that your parents are people too. Not just chaffeurs, laundresses, baseball-catchers, etc.– but people. And when that happens, it is a lightbulb moment, a moment in which a parent’s humanity, flaws, and individuality come into focus.
If you are lucky, like I am, you get a window into that world via an adult relationship with your parents. In this domain you start to learn more about them; you see them through the eyes of their friends, their employer, their spouse, and their other children.
Yesterday I sat transfixed reading Katherine Rosman’s book If You Knew Suzy: A Mother, A Daughter, A Reporter’s Notebook cover to cover. The book arrived at noon and at 11:00 last night I shut the back cover and went to sleep. But by the middle of the night I was up again, thinking about it.
I had read an excerpt of the book in a magazine and had already been following Katie on Twitter. I knew this was going to be a powerful book for me, and I was right. Katie is a columnist for The Wall Street Journal and went on a mission to learn about her mother after her mother died in 2005 from lung cancer. In an attempt to construct a completed puzzle of who her mother was, Katie travels around the country to talk with those who knew her mother: a golf caddy, some of her Pilates students, her doctors, and even people who interacted with Suzy via Ebay when she started buying up decorative glass after her diagnosis.
Katie learns a lot about her mother; she is able to round out the picture of who her mother was as a friend, an inspiration, a wife, a mother, a strong and humorous woman with an intense, fighting spirit. These revelations sit amidst the narrative of Katie’s experience watching her mother going through treatment in both Arizona and New York, ultimately dying at home one night while Katie and some family members are asleep in another room.
I teared up many times during my afternoon getting to know not only Suzy, but also Katie and her sister Lizzie. There were so many parts of the book that affected me. The main themes that really had the mental gears going were those of fear, regret, control, and wonder.
I fear that what happened to Suzy will happen to me:
my cancer will return.
I will have to leave the ones I love.
I will go “unknown.”
My children and my spouse will have to care for me.
My needs will impinge on their worlds.
The day-to-day caretaking will overshadow my life, and who I was.
I will die before I have done all that I want to do, see all that I want to see.
As I read the book I realized the tribute Katie has created to her mother. As a mother of three children myself, I am so sad that Suzy did not live to see this accomplishment (of course, it was Suzy’s death that spurred the project, so it is an inherent Catch-22). Suzy loved to brag about Katie’s accomplishments; I can only imagine if she could have walked around her daily life bragging that her daughter had written a book about her… and a loving one at that.
Rosman has not been without critics as she went on this fact-finding mission in true reporter-style. One dinner party guest she talked with said, ” … you really have no way of knowing what, if anything, any of your discoveries signify.” True: I wondered as others have, where Suzy’s dearest friends were… but where is the mystery in that? To me, Rosman’s book is “significant” (in the words of the guest) because it shows how it is often those with whom we are only tangentially connected, those with whom we may have a unidimensional relationship (a golf caddy, an Ebay seller, a Pilates student) may be the ones we confide in the most. For example, while Katie was researching, she found that her mother had talked with relative strangers about her fear of dying, but rarely (if ever) had extended conversations about the topic with her own children.
It’s precisely the fact that some people find it easier to tell the stranger next to them on the airplane things that they conceal from their own family that makes Katie’s story so accessible. What do her discoveries signify? For me it was less about the details Katie learned about her mother. For me, the story of her mother’s death, the process of dying, the resilient spirit that refuses to give in, the ways in which our health care system and doctors think about and react to patients’ physical and emotional needs– all of these are significant. The things left unsaid as a woman dies of cancer, the people she leaves behind who mourn her loss, the way one person can affect the lives of others in a unique way… these are things that are “significant.”
I woke up in the middle of the night thinking about the book. My head spun with all of the emotions it raised in me. I think that part of the reason writing has become so important to me is precisely because I do realize that we can die at any moment. And if you don’t have an author in the family who might undertake an enormous project as Katie did, where will that explanation of who you were — what you thought — come from?
Is my writing an extension of my desire to control things when cancer has taken away so much of this ability?
Is part of the reason I write an attempt to document my thoughts, my perspective for after I am gone… am I, in a smaller way, trying to do for myself what Katie did for her mother?
If I don’t do it, who will do it for me?
And in my odd way of thinking, am I trying to save anyone the considerable effort of having to work to figure out who I was– deep down?
[My original blog had] the title “You’d Never Know”: I am telling you things about myself, my worldview, and my life, that you would otherwise have no knowledge of. One of the things people say to me all the time is, “You’d never know to look at you that you had cancer.” After hearing this comment repeatedly I realized that much of our lives are like that:
If we don’t tell someone — share our feelings and experiences — are our lives the proverbial trees falling (unheard) in the forest?
What if you die without being truly understood?
Would that be a life wasted?
If you don’t say things for yourself can you count on others to express them for you?
Further, can anyone really know anyone else in her entirety?
After a loved one dies, there always seems to be at least one mystery person: an individual contacts the family by email, phone, or in person to say, “I knew her: this is how I knew her, this is what I remember about her, and this is what she meant to me.” I know that this happened when Barbara (my beloved mother-in-law) died suddenly in 2009. There are stories to be told, memories to be shared. The living gain knowledge about their loved one. Most often, I think families find these insights comforting and informative.
Katie did the work: she’s made a tribute to her mother that will endure not only in its documentation of the person her mother was (and she was quite a character!) but also in sharing her with all of us. Even after her death, Suzy has the lovely ability to inspire, to entertain, to be present.
I could talk more about the book, Katie’s wonderful writing, and cancer, but I would rather you read it for yourself. I’m still processing it all, making sense of this disease and how it affects families, and being sad that Katie’s children didn’t get to know their grandmother. Katie did have the joy of telling her mother she was pregnant with her first child, but Suzy did not live long enough to see her grandson born. In a heartwarming gesture, Katie names her son Ariel, derived from Suzy’s Hebrew name Ariella Chaya.
I thank Katie for sharing her mother with me, with us. As a writer I learned a lot from reading this book. I had said in years prior that “we don’t need another memoir.” I was wrong. That’s like saying, “I don’t need to meet anyone new. I don’t need another friend.” Truth is, there are many special people. Katie and Suzy Rosman are two of them.
November 18th, 2013 §
 I’ve never forgotten seeing the black and white cow with a window carved into its side. I was in grade school, living outside of Milwaukee, and always loved going to the Wisconsin State Fair each summer.
I’ve never forgotten seeing the black and white cow with a window carved into its side. I was in grade school, living outside of Milwaukee, and always loved going to the Wisconsin State Fair each summer.
There was a beautiful cow lazily eating in a pen, indifferent to all of the people milling about.
When I walked around the enclosure to see its opposite side, however, the cow was anything but normal-looking. The cow’s left side had a glass-covered hole in it. The man standing next to it and stroking its head was talking about cows’ digestion. He said the window allowed access to the cow’s stomach for research about nutrition and illnesses. The man then shocked the audience by opening the cover of the hole and reaching inside the cow’s upper stomach to extract a handful of grass that was in the process of being digested. The cow remained aloof.
I have now learned that the cows are called “cannulated cows” or “rumen-fistulated cows.” I have been able to confirm that my memory of seeing one at the Fair is correct. As I remember it back then, the window looked more like a miniature glass dryer door, one that swung open with a small hinge on one side. I am not sure of that. The photos I see of cannulated cows now have a different look. To learn more about rumen-fistulated cows you can watch this video which is extremely interesting.
I woke up thinking about that black and white windowed cow this morning.
I woke up wanting a window into my body and what is happening inside right now, this very minute. I want to know if the clinical trial I’m participating in is having any effect on my cancer. For now we use other indicators but they are unreliable. Even blood tests for tumor markers lack validity and reliability in many people (why they are not used as screening tools to diagnose breast cancer in the general public).
And so I forge ahead, taking pills, getting injections, wondering if it is doing anything to keep my metastatic breast cancer under control. Side effects vary day by day. Yesterday was a bad day. Terrible back pain, gastro issues, a migraine, and fatigue had me down for most of the day. But today I feel better.
So I focus on today.
I envy the researchers who gain knowledge in real time. I envy the way their information can be analyzed and promptly used to help sick cows.
I wish I had an immediate view inside, an indicator as to what my body is doing. Instead, the image of the black and white cow with the window in its side stays with me.
November 14th, 2013 §
 Tuesday was a full day for me at Memorial Sloan-Kettering for Cycle 1, Day 16 of my current clinical trial.
Tuesday was a full day for me at Memorial Sloan-Kettering for Cycle 1, Day 16 of my current clinical trial.
With snow flakes and rain mixing in the morning rush, I decided to skip the train and go early with my husband as he made his usual morning commute to New York City by car. I knew this would get me to the office quite early. I was the first to arrive in the waiting room and didn’t mind the long wait. It gets very busy and noisy later in the day and I’m always happy to sit in warmth and comfort of a quiet room. I arrived at about 7:20 and my first appointment wasn’t scheduled until 8:30. I was fasting, so I did miss my morning coffee quite a bit while waiting, though, especially as other patients began to arrive and use the coffee machine!
I meet with the research nurse first. She weighs me (down 2 pounds from two weeks ago), takes my blood pressure (oops, very high using the machine, we’ll retake it manually, oh that’s much better, thank you very much), pulse (in the 90s), oxygen saturation (better than last time, now normal).
We review how I am feeling on the Faslodex and GDC-0032 combination. This is the first time I am discussing it with the team since starting the protocol. She goes through a list of symptoms and asks about each one. The list ranges from gastrointestinal issues (very important to monitor on this investigational drug) to neuropathy to dizziness to fatigue to rash. I am pleased to report that I feel quite good on the combo. I experienced a few days of hot flashes and night sweats from the first injections of Faslodex two weeks ago, I tell her, but that was it. From the GDC I really only have had appetite loss, metallic taste in my mouth, a bit of muscle pain, and slight fatigue as the most noticeable issues. In general, we both agree, I am tolerating it very well.
The biggest change I’ve experienced in the last two weeks is a drastic change in my breathing– for the better. I’m quite sure, I tell her, that my pleural effusion (excess fluid in the lining around the lungs) is almost resolved. This is great news and I am anxious to find out if my doctor hears the change. I also tell her that after much thought I have decided to have a port placed to make my blood draws and tracer injections for CT and bone scans easier.
Next I meet with my own oncologist. Usually I would meet with the Principal Investigator for this appointment. She was not in the office on the usual days this week, though, and I must have my check-ins on certain days in the cycle. I was told about the switch in schedules well in advance. The plan for the long term anyway is that I will transition back to my own oncologist for monitoring. The two doctors work closely together and there is no problem in doing this.
I haven’t seen my oncologist in what seems like a while (probably about one month) and we are happy to be “reunited” for this appointment. We review how I am doing clinically. She also gives me a physical exam and listens to my lungs. Yes, she agrees, there is a big change for the better. We discuss the port, and she orders the needed additional bloodwork for it.
We talk about the trial and other topics. As always, she asks about my family and writing. I tell her about the song I wrote and promise to send her a link to it. I tell her I have been invited to come talk to the class of Fellows at Sloan-Kettering in a few weeks about caring for the metastatic breast cancer patient. I am truly excited about this invitation. There isn’t anything I can think of that is more important than talking to young physicians about ways to make doctors and patients partners in care in light of a metastatic cancer diagnosis. I’ll share more about that visit as the time approaches.
Next I do scheduling for the next appointment in 2 weeks. That will be a much shorter day than today. Each appointment in the first 8 weeks on the protocol has different elements. Today will be a long day. Next time will just be a visit with the Principal Investigator and a blood draw.
 Next I head upstairs to the chemo suite where they have a room waiting for me. They have already called downstairs while I am doing scheduling to tell me which room to go to so I don’t even need to check in. The nurse I had last time comes in to the chemo room. I immediately tell her that she did a wonderful job with the two huge injections of Faslodex last time. I tell her the slow injection rate seems to have worked; I was sore for days (expected) but no bruising or welts. I always try to give as many compliments as I can; I think these oncology jobs must be very stressful and I would bet the complaints come often. If possible, I try to find something good and comment on it. Everyone likes being appreciated.
Next I head upstairs to the chemo suite where they have a room waiting for me. They have already called downstairs while I am doing scheduling to tell me which room to go to so I don’t even need to check in. The nurse I had last time comes in to the chemo room. I immediately tell her that she did a wonderful job with the two huge injections of Faslodex last time. I tell her the slow injection rate seems to have worked; I was sore for days (expected) but no bruising or welts. I always try to give as many compliments as I can; I think these oncology jobs must be very stressful and I would bet the complaints come often. If possible, I try to find something good and comment on it. Everyone likes being appreciated.
Today I will need to have my blood drawn, take my GDC-0032 pills, wait four hours, and have my blood drawn again. I must always wait one hour after taking the pills to eat. By the time I do all of this today it will be noon. The nurse gets a vein in my wrist easily for the required 12 vials and when we see it’s a good flow we agree to leave the line in and try to use it four hours from now and avoid another stick. I’m reactive to adhesive so she wraps me up carefully and I slide my sweater sleeve back down.
I take my pills with a full glass of water and document the time in the medication diary that I am required to keep. Then it’s time to drop my trousers for the two big Faslodex injections. I am not too nervous about this part now that I’ve done it once already. I will get these today, again in two weeks, and then monthly thereafter. I have mastered the art of muscle relaxation for these shots and use a trick of putting all of my weight on one foot while they inject the opposite side. Again the shots are uncomfortable because the viscous liquid is getting rammed into a muscle. But she does it slowly again as she is supposed to, and we’re done quickly. I still am self-conscious as the lightly-frosted sliding glass doors are all that stands between my tush and the hallway, but I’m already over that. I think the idea of facing the wall and clutching a table as needles are jabbed in my backside is probably more laughable.
I put on my coat, knowing the worst is over for the day and go meet a friend for lunch after waiting the required time to eat.
Later, I return directly to the same room I was previously in at the appointed time. The line still in my wrist yields a good flow, a few more tubes are drawn, and we’re done for the day.
Seven hours after first entering the building I am free to go. I still have two more weeks’ worth of the GDC-0032 in my bag and so I do not need to visit the pharmacy. At the next visit my medication log will be checked and my remaining pills will be counted and confiscated before I am given another 30 day supply.
…….
Over the last two days I have ended up needing two more blood draws, met with my local oncologist, and got my monthly Xgeva shot. After 7 needles in 3 days I’m glad to now have a few days off. I ended up needing to repeat one of the tests required for the port placement procedure (Tests related to clotting are routine before any surgical procedure. One of these was slightly elevated and I needed to repeat it. The second test came back just fine).
I also had my tumor markers done. This blood test is not a part of the clinical trial requirements. I’ve decided to watch these to see what they do while taking the drug. I’m sure some people would not choose to do this. This week’s test showed the numbers were quite elevated over previous weeks. We don’t know what that means. I have no increased pain, none of my other bloodwork shows any reason for concern. The numbers sometimes rise on new therapy before they drop. My breathing is significantly improved. So, we focus on the clinical signs and will just have to see what the markers do. I wish they had dropped, but I’ve seen the imperfect nature of this test time and again. I am able to realize this is only one piece of the puzzle right now. It doesn’t affect anything about my treatment plan. A reminder: in this trial success is measured by doing CT scans at varying intervals. My first one will be five weeks from now, at the seven week mark. Only then is a determination made about whether it is working, which would be disease stability or reduction. If the overall “quantity” of cancer is seen as growing by 20% or more, I would discontinue the trial and need to move to something else; it would be considered ineffective for me.
I was sore far more quickly after the Faslodex injections this time even though they weren’t any more painful at administration time. By the time I was on the train back home in the late afternoon I was hurting. For three days now I’ve had a heating pad on as much as possible. It just feels good. The seat heater in my car is getting a workout too. I know it will only be another day or two so I am not too bothered.
I don’t yet have a date scheduled for the port placement. That could be as soon as next week. I also have meetings with my cardiologist (these inhibitors can drastically change lipid levels. My cholesterol and triglycerides on my previous drug, Afinitor, went quite high. Thankfully they are coming down rapidly now but we still need to watch them carefully.) and my endocrinologist (my thyroid levels are now abnormal again. I have Hashimoto’s Disease which is usually very easy to manage but chemo does sometimes cause changes). I’m not in a huge rush to get the port, I just would like to have it in by the time I need to do the next round of scans.
I’m glad to finally be done for the week with appointments, hard to believe the weekend is almost here. I will see what next week brings and then it will be time to be back at MSK on the 25th of November for Cycle 2, day 1.
November 11th, 2013 §
 Today is Veterans Day.
Today is Veterans Day.
Each year on this special day and Memorial Day my letter to troops stationed overseas is similar. Each year I question whether I should write something new, if it’s “cheating” to say the same thing. In the end I realize that thank you never gets old, it never needs to be re-written. Thank you doesn’t have an expiration date.
November 11, 2013
Dear Servicemen/women,
My family and I want you to know that we have not forgotten you or the sacrifice you are making every day to be away from your own families and in harm’s way. It’s not much, but perhaps knowing you are in our hearts and minds will help.
Six years ago I was diagnosed with breast cancer. I was in remission for more than five years and now my cancer has metastasized to my bones and lymph nodes. It is not curable.
As I go through treatment, people called me brave. I don’t think I deserve it. “Brave” is not a word you used about someone like me. I have gotten cancer by chance and I am dealing with it, the best I can.
But soldiers? You are brave. You have a choice—you put your lives on the line after making a conscious decision to do so. You know the danger and you do it anyway. To me, that is true bravery, true heroism.
Seeing danger and making the choice to proceed anyway is precisely how I define bravery. We all find ways to deal with the fear of death. We know the uncertainty that lies ahead. We see the bravery in others before we will see it in ourselves.
What underlies bravery: chance or choice? Can both?
Are we just hesitant to see the quality in ourselves? Are we just modest? Do we just act the way we need to, to get the job done?
I think when you choose to throw your hat in the ring, that choice counts for something.
That makes you brave.
That is what makes soldiers heroes.
To all of our veterans, thank you for your continued service to our country.
Lisa Bonchek Adams
(The photo above is of a needlepoint project I started work on long ago. Instead of doing a traditional flag I decided to stitch it as a sampler. It is obviously only partly finished but I love how it ties in to this post.)
November 7th, 2013 §
Yesterday there was a video of a woman throwing a dance party in the operating room on the way in to her double mastectomy. The headline called what she did “awesome” and the writer of the piece said she wanted to go clubbing with the woman after she “was all healed.”
The video went viral. Many people thought it was, as the headline had said, “awesome.” The piece called her “brave.”
So what’s the problem?
I have no judgment on the woman who had the dance party. You want to shake your booty to Beyonce before you go off to dreamland for cancer surgery? If your surgical team feels it doesn’t compromise anything about the environment, go for it.
But why a video of this goes viral and everyone cheers “Awesome! Brave!” … well, the implication is that if you didn’t do that as you went in to your double mastectomy, you’re not awesome. Or brave.
On the morning of my double mastectomy in 2007, I packed my two older children off to school after making sure they had warm hats and gloves, typed out a schedule for those would be taking care of my children while I was in the hospital for a few days, reluctantly left my third child (only seven months old), went to the hospital, got prepped for surgery and laughed with my surgeon as he (unnecessarily, it seemed to me) signed both of my breasts with purple Sharpie to indicate which body parts needed to be removed.
True awareness means showing the spectrum of what experiences are like for people with breast cancer, and not making them feel less than “awesome” if they don’t want to dance into their operation and just want to be wheeled in as usual. Videos of dancing patients reinforce putting a carefree, happy face on a disease that — even if detected early– still has a 20-30% chance of metastasizing, sometimes decades later.
I did everything possible to keep my cancer from returning. But it did anyway. I now have stage IV breast cancer, a diagnosis considered incurable.
I am no less awesome just because I didn’t dance and sing when they wheeled me in to surgery six years ago. I smile and laugh and write on my blog many days a week to educate and inform readers. But that isn’t as “fun” as showing a video of a dance session in the OR. I think the way we all rally to treat this disease deserves recognition.
There are many ways to be inspirational, and they don’t all involve flash mobs in the operating room. Unfortunately, however, feather boas and booty dances are the stories that get the public’s attention.
November 6th, 2013 §
 Even when I am alone
Even when I am alone
I teeter precariously over the right hand side of the bed.
On my left shoulder when I can,
When the pain is bearable,
When I can settle in for the night.
I still approach the precipice
Rather than opt for the safety of the middle place.
I act as if he is there with me
Taking space
And I, trying to make room,
Move to outer orbit,
As if that extra inch or two would matter.
Even on the occasions I am alone
I pretend as if I am not.
I go to places in my mind,
Wondering what it will be like
When that opposite side of the bed is empty
For him
And he teeters precariously near the edge unnecessarily,
Without me there to take up space.
November 2nd, 2013 §
 Finally! After months of writing, recording and mastering, Doug Allen and I have released the song Six Minutes for distribution.
Finally! After months of writing, recording and mastering, Doug Allen and I have released the song Six Minutes for distribution.
It is on iTunes here or you can get it here via CDBaby.
We are really proud of it and grateful to so many people who helped us with it… Donna Bonato at Silver Creative for turning one of my garden photos into the stunning cover art, Dennis Hrbek for his sound work, Anthony Radice for piano and some initial recording tracks, and of course our families and friends for their support along the way.
The background of the song as I wrote it for distribution is this:
I’ve been writing on my blog about my life for a few years and more recently about my diagnosis in 2012 with stage 4 breast cancer (6 years after initial surgery and treatment). Many of the posts I make are more poetic than prose lately. One particular one called “No room for that in this (Six Minutes)” seemed ripe for becoming song lyrics. I’ve never written song lyrics before and don’t even sing or play an instrument. But I did think the words had some potential to tell a good story, something I think is lacking in so much of modern music.
I’m a huge fan of Doug’s personally and professionally. He’s been teaching our son Colin to play guitar for a few years now. We’ve become friends and I love Doug’s sound. After hearing his latest album I knew he was someone who would be able to find the right music. I knew that on occasion he would co-write songs. I asked him, on a lark, if he’d consider working with me on turning the post into a song. He agreed.
We sat at my kitchen table and in that first session I turned that original post into the lyrics for “Six Minutes.” Doug almost immediately got the right feel and sound for the music and it just clicked. We both felt that while the original storyline of the song was about me, the song itself needed to be more universal. That’s why I made the chorus something so approachable, something everyone can relate to.
For me, the six minutes were ones of pain that I wanted to go by quickly. But I regretted that I was wishing my life away in these small increments. What Doug and I knew for sure is that we all can relate to the idea of “taking a trip inside your head” where you just check out during the day. That’s what he and I kept coming back to. Daydreaming, zoning out, whatever it is that helps you take a little break. So the chorus is about that, which is important because those are the words you’re likely to be singing to yourself again and again and need to be able to relate to.
The song came together very easily for us. The words really didn’t change after that first meeting. I think we knew we had the right music for it and the story is now there for sharing.
We hope listeners will enjoy it, we hope it will speak to them. This one is a true collaboration and I’m grateful Doug was able to share my words in a new way. After hearing it hundreds of times now I still find myself singing the chorus again and again at moments throughout the day.
You might enjoy seeing that original post and what the lyrics became in the final version…
Six Minutes
The clock says it’s been six minutes now,
I’m glad that they have passed,
Then I realize I’ve wasted them:
Six minutes gone too fast.
I take a trip inside my head,
I don’t know where I go.
Somewhere else,
Anywhere else,
Far from things I know.
I try to forget for a moment now,
Focus on a spot on the wall,
I lose myself in the emptiness,
Such a painfully long way to fall.
So I take a trip inside my head,
I don’t know where I go.
Somewhere else,
Anywhere else,
Far from things I know.
I find myself in silence,
Tuning out the noise,
No room for anything,
But him, my girl and the boys.
And when I’m gone,
Just no way around it,
So many things they will miss
‘Cause when it comes to being fair,
There’s no room for that in this.
Gonna take a trip inside my head,
I don’t know where I’m gonna go,
Somewhere else,
Anywhere else,
Far from things I know…
October 30th, 2013 §
 There is so much to say about the start of the phase 2 clinical trial earlier this week. I think it’s important to be as complete as I can on the main parts. I really want readers to get a sense of what it’s like to go through this and also what to expect if they decide to enter a trial themselves.
There is so much to say about the start of the phase 2 clinical trial earlier this week. I think it’s important to be as complete as I can on the main parts. I really want readers to get a sense of what it’s like to go through this and also what to expect if they decide to enter a trial themselves.
That said, it is obvious to me (and hopefully to you) that my experience is very unique. I have no earthly clue what other trials are like. I just want to make all of the disclaimers that I think you all know already: this is my experience only. If that helps in some way, great. But it can’t possibly tell you what another clinical trial might be like.
I still think it’s valuable. And I know I would have wanted to read posts like these a few weeks ago when I was signing up for the trial. So that’s my guide: if I think it would have helped me, I’m going to share it.
Twitter friends have been telling me that they are interested in five main topics: 1) what is the science behind this drug? 2) what does the treatment consist of/logistics 3) how did I choose this trial out of the ones available 4) side effects physically 5) effects emotionally. The last two will obviously be the ones we follow over time. I won’t be able to address all of those topics here but I’m getting a good jump on them.
This post is long. I’ve opted to just publish it and not divide it up. If you want to read it in chunks you can decide how to divide it up. If you want to skim the science parts, you’ll still have my report of my day at the end. I look forward to hearing your questions and comments. If you have questions I will try to answer them.
First, a bit about the drugs and the science behind them. My trial has me taking 6 mg of an investigational drug called GDC-0032 made by Genentech every morning. I receive two injections of a drug called Faslodex every month, with an extra dose halfway through the first month.
It is important to understand that these particular drugs for metastatic breast cancer are not traditional (cytotoxic) chemotherapy drugs. What I mean by that is that most people think about chemo as being drugs you receive, most often via IV, that makes you feel rotten and your hair fall out. That’s the type most people are familiar with and that class of drugs includes what I had when I had treatment for stage II breast cancer in 2007 (Adriamycin, Cytoxan (least creatively-named drug of all), and Taxol).
Those drugs are cytotoxic (cyto= cells, toxic= poisonous). So, the drugs kill the cancer cells but they kill other cells too. That’s why your hair falls out, you feel sick, your blood counts drop and a host of other issues.
With my kind of cancer (estrogen receptor positive, progesterone receptor positive, HER2 negative) there are other types of drugs to use to try to slow the cancer’s growth down. This is not the case for all types of breast cancer. With some you can only use traditional chemotherapy. In addition, and most importantly for this trial, my cancer shows a mutation in the Pi3k pathway. I know this is getting very science-y. But I’ll try to explain the rationale for this drug.
Many people with my kind of breast cancer (and other types of cancers, we’re learning) show a mutation in this pathway. You might have heard of genomic sequencing. It is testing the tissue of your cancer to see if your particular cancer has any mutations in its coding that facilitate the cancer’s growth (I’m oversimplifying here). This pathway, which is called the Pi3K/AKT/mTOR pathway, can become overactive and drive the cancer’s growth.
I have one mutation in the Pi3k section of the pathway. There are many forms of mutations in the Pi3k pathway. There can be other mutations in other areas as well. Mine is called a Pi3k-alpha mutation.
So what the investigational drug is targeted to do (hence the term “targeted therapy”) is to block this Pi3k/AKT/mTOR pathway that has been over-activated, potentially by this mutation.
This all sounds great. But it’s not so easy. It isn’t as easy as “find the mutation, create the drug, block the pathway, cancer goes away.” We don’t have indications it will ever be like that. The signaling pathways of cancer are highly complex, variable at any given point, and also change over time.
In addition, not everyone with the same mutation responds to the same drug. And combinations of drug seem to work better. Think about doing clinical trials of endless permutations of drug combinations with different mutations, different cancers, in different bodies… well, this is why science seems to move at lightning speed but our advances in treatment just don’t mirror that in all cancers. We have no way at the moment to predict what the best course of treatment is for any individual person. For now, you throw the pasta at the wall and see if it sticks. Unfortunately, our lives are the test cases.
To return to the science, I’ve already tried an mTOR inhibitor in my last treatment phase. That was called Afinitor (combined with another drug called Aromasin). But that targeted a different end of the pathway, and not the mutation. The problem with all of these right now is that the cancer figures out a way around the blockages. It develops feedback loops. If you’ll allow me to anthropomorphize cancer for a minute, it says, “Hey, okay, so you want to block the road? I’ll just detour and still get the end point. I’ll get fuel to the cancer somehow. If you block me, I’ll just keep finding a new way to deliver the goods.” And that’s why metastatic breast cancer is incurable. It keeps finding a way to find fuel and becomes resistant to each thing you throw at it. I became resistant to that Aromasin/Afinitor combination after about six months.
In terms of side effects, unlike traditional IV chemo, with this investigational drug you don’t “feel rotten” right after treatment. It can take weeks and potentially months for side effects (especially some of the serious ones) to take hold. So that’s one way this differs from what people might think. My phone has been buzzing non-stop since Monday: “How do you feel? How do you feel?” I will have some effects from the injections (which are hormonal agents, this one is an estrogen receptor agonist) quickly. I already have some of those. Other side effects from the pills (the GDC-0032) will come later.
So… here we go.
Monday was Cycle 1, Day 1.
If you are interested, my trial protocol is here (I am in the phase II group). This tells you exactly what this study is. If you want to read a bit about the early results of this drug in phase 1 trials you can see that here.
On day 1 I received my GDC-0032 pills for the month (and took the first dose), received two injections of Fulvestrant (Faslodex), and had about 8 vials of blood drawn.
The logistics of getting to the city were a bit of a challenge this week given fatigue and the lingering pleural effusion. The train, subway, and walk were tough but I always try to push myself. Knowing I’d be stuck inside for a few hours definitely had me enjoying the cool crisp fall air on the walk to the hospital.
Because of train times I arrived one hour early for my appointment. I wasn’t sure if I was doing this blood draw before seeing the doctor or after so I settled in. After only a few minutes I was surprised to be called back to an exam room. There I had a long meeting with research nurse whom I’ve spoken with by phone but not met in person. It was an extremely thorough meeting. She answered questions, reviewed the protocol, went through my current medications again, noted all physical symptoms I’m having now. We also discussed my most recent bloodwork (my lipids changed drastically during the 3 week washout period. My prior chemo had raised my cholesterol significantly. My LDL dropped a whopping 100 points in a two week period once I stopped the old chemo, for example). Blood pressure, pulse, oxygen saturation, height, weight. Other research assistants on the protocol come in and talk to me, discuss things, physical exam, as eventually does the Principal Investigator (the doctor in charge of the trial).
It took about two hours to complete these meetings, exams, tests, questions, medication review, etc. Everyone was very thorough and I was offered every opportunity to ask questions about not only the trial but also about any symptoms I was having and how they could be helped.
They also stressed how important it is to call with any and all side effects. As the more serious side effects become more possible/likely, it’s important to report any issues right away so they can be managed before they get too serious. Communication is key in clinical trials. I’ll talk about the side effects more in the future.
For some questions about side effects we needed to refer to the protocol of the trial (Can I get radiation to a bone if my bone pain continues: Yes, but not within the first two weeks of the trial start. Can I get the fluid around my lung tapped if it becomes too troublesome: Yes, at any time).
We also discussed a port for my blood draws/access for radioactive dye injections for CT and bone scans that I will need to have done every 8-12 weeks on the trial. I am still undecided about the port. We agreed to see how it goes in the next few weeks with the blood draws. I can only use my right hand which doesn’t allow for easy access or many misses. They tell me there is a “three miss rule.” If they can’t get the blood they need within three tries, they stop. I have a terrible feeling this rule will come in handy.
At the end of the meetings they handed me many sheets of paper.
First, I received a medication diary where I need to document the time I stop eating every night and the time I take my GDC-0032 pills (the “investigational drug”) the next morning. The pills must be taken on an empty stomach one hour before food, with a full glass of water at approximately the same time every day.
Second was a list of drugs and supplements I cannot take while I am on this protocol.
Finally, there was a schedule for the next 8 weeks of what will happen at each appointment, what tests and drugs I will receive, what I need to do to prepare, and what I need to bring to each appointment. The pills are given in quantities of 30 but I will probably be at appointments every 28 days. The surplus pills must be traded in and counted before I can receive the next month’s supply. Though it is only one drug it is dispensed in two capsules, one dark red, one pine green. One is a 5 mg, one is a 1 mg for a total of 6 mg.
I was then sent to do scheduling for my next appointments. I will need to return in two weeks (plus or minus 2 days) to do vital signs, exam, fasting blood draw (but this time it must be done twice: before taking my pills and then again 4 hours after), and my two injections.
I then went to the hospital pharmacy to collect my pills. They are labeled with my name, the drug name, instructions, and so on, just like a regular prescription. The protocol number is labeled on the bottles too. The bottles also say “Cost $0.00” on them.
This drug is provided free of charge to me but my insurance company is billed for the injections of Faslodex, lab work, and all scans. Trials differ in what is covered. In this case, only the investigational drug is provided free of charge. The rest of the expenses including the visits with the doctors are not provided for free. I am fortunate. My insurance will help pay for those things. Your care is not necessarily fully covered when you are in a trial, contrary to popular belief.
The pharmacy cashier placed the two bottles (one bottle of the 5 mg, one bottle of the 1 mg) in a brown paper lunch bag and handed it to me. In that moment I feel like I have something very valuable and secret in my possession, perhaps even magical. I don’t know if these pills will do anything for me. They could do me more harm than good. They could do nothing. But they might buy me time. Those are, for now, mysteries.
The brown paper bag with the drug bottles inside seems very wrong, far too flimsy for the weight of the hope that lies within.
I then left the pharmacy and headed upstairs to the chemo floor where I had my fasting bloodwork done (by now it was past 11 AM and I was glad I started early. I really don’t mind not eating, it’s the lack of coffee that gets me. Also, the longer I wait the harder the blood draw is likely to be).
In this room I will also receive my two injections. As I enter the room, I’m wondering about those and anxious. The number of needles I have in a month is astounding sometimes. I was the girl so afraid of shots as a kid I once ran into the parking lot to try to run away to avoid getting a vaccination at a pediatrician’s visit.
One chemo room is dedicated to this trial. I have gone to the same room each time so far. The trial tech doesn’t even try to draw my blood. He calls in the reinforcements. Eight or so vials of blood are taken by a nurse who goes after my hand vein with a vengeance. Unfortunately I receive a call the next day that two of the vials are unusable (hemolyzed). This happens sometimes when large blood draws require a lot of work (suction) to get. I was able to go locally the next day to have the two vials redrawn.
After the blood draw it was time for the “standard of care” drug. This is part two of my clinical trial protocol. The “standard of care drug” means I am given not just the experimental drug, but also a drug that is a reasonable option for treatment for this stage of my disease.
On its own (“single agent”) Faslodex works for some people but seems to have a better track record when combined with another agent. My trial is one that combines Faslodex injections (standard of care) with the GDC-0032 (the investigational drug). There is no placebo. This is a phase II trial. I will get both. We will see if taking the GDC-0032 provides a better result than the historical success rate of those who have received the Faslodex injections alone. There will be 60 people nationally doing this combo, about 10 of them at Sloan-Kettering. I am the fourth person, I believe, to get started on it (the trial just opened a few weeks ago at Sloan).
Faslodex is given by injection, intramuscularly, in your rear. No fancy fun way to say it. You drop your trousers and they have syringes that are over 4″ long (can’t find any literature that states exact measure. I’m going to ask to measure it after my shots next round. I confess I saw them when we were done and they made me a bit nauseated and I didn’t want to be precise!). The needles are thick because the liquid that has to be inserted is very viscous and doesn’t go into the muscle easily. I was fortunate and the nurse did a great job. I tried to remember the tip to keep your muscles relaxed during an intramuscular injection, but it’s hard when you know the size of the needle that’s taking aim for your ass.
The first injection really wasn’t worse than a regular shot. The second one hurt more than the first but still less than I had expected. I opened my bottles of pills, took out one of each, drank my water as directed. I noted the time in the diary.
At this point I was free to go. The injection sites were not immediately painful and I was sent on my way.
Everything was incredibly efficient and while I was exhausted, I was relieved. I kept thinking to myself: “Once again after three weeks of not being actively treating my cancer because of the mandatory ‘washout’ period, I am doing all I can. Action feels good.”
I celebrated getting through day 1 by having lunch with my friend Julie Klam which was such a luxury after the poking and prodding of the morning. I took the train home and felt a sense of accomplishment.
So, in case it wasn’t clear, my next appointment will be two weeks after my start date (“Cycle 1, day 15 +/- 3 days” in protocol speak.).
I think the word that most defines metastatic breast cancer to me is “uncertainty.” You have to figure out a way to live with it. My coping mechanisms are research and action. I can only hope these will serve me well.
I thank you for your support and encouragement this week.
October 26th, 2013 §
 I know I shouldn’t always attach explanations on posts like this but today I feel the need to. Whenever I post a dark piece I get many messages of concern (and criticism) from people. Sometimes they say “Lighten up.” Most often readers are worried. I want to say that these pieces capture only a fraction of the spectrum of feelings I have.
I know I shouldn’t always attach explanations on posts like this but today I feel the need to. Whenever I post a dark piece I get many messages of concern (and criticism) from people. Sometimes they say “Lighten up.” Most often readers are worried. I want to say that these pieces capture only a fraction of the spectrum of feelings I have.
My days are not spent wallowing in sadness. When I need to rise to the occasion I do. It’s often easier for me to write about the world of the dark places though… in some ways I think those are the ones that need light the most. These words are often the ones which go unwritten and unexplored.
I always find joy in the small moments each and every day. Today I tweeted, “I find beauty in the flowers in my room, the sight of the leaves through the window, the sound of the wind, the loyalty of my dog.”
There is shimmer in each and every day. Some days we just have to look hard for it, dig deep. And some days there is just a darkness overhead. I find that giving a voice to the those depths, shedding light on them, is important. There are many who live in this land. Today’s post comes from the feeling of doom that accompanies test results, that awful waiting period.
………………………
I wait for the burlap bag over my head,
Wait for the rope round my neck.
I wait for the chair to be kicked out,
The floor to drop open,
Snapping the rope’s length and my body with it.
This is what it feels like each time I drive to the office,
Head into the building,
Take a seat.
Usually I hate traffic
But when it slows my journey I find myself grateful these days.
Stretch out that time.
Make it longer until I hear words I don’t want to hear.
They are tricks, of course,
Silly childish games I play.
I turn on the heated seat and press my back against the core
Burning relief into my spine.
I am at war with myself.
I ready myself to smile, to say good morning,
To greet the office staff with a brave and carefree smile.
“How are you?” one will ask,
Letting the words roll off her tongue the same way
The lady with the Irish accent ringing up my groceries asks me
Without waiting for an answer.
I’m not fine.
I’m anything but.
There is no time for that, though.
It’s time for results and plans and tests and exams.
It’s time to steel myself again,
Stand up straight,
Pretend there is no fear,
No ache,
No catastrophe.
For minutes at a time this is how I get through the day.
I walk at a clip, slightly faster than that executioner with the bag and rope who chases me,
One step behind or maybe two,
Telling him
No.
Not today.
Just stay the hell away from me.
Just for a little while longer.
October 18th, 2013 §
 I confess I have putting off writing this post. After getting results of my scans I needed a few days to just sit with the information. I have also been dealing with some physical issues during my washout period (an interval where you must be chemo-free) before my clinical trial starts on October 28th.
I confess I have putting off writing this post. After getting results of my scans I needed a few days to just sit with the information. I have also been dealing with some physical issues during my washout period (an interval where you must be chemo-free) before my clinical trial starts on October 28th.
I had CT scans of my chest, abdomen, and pelvis. I also had a bone scan of my body. I had bloodwork and an EKG and a urine test. These are all tests that need to be done before I can start the clinical trial and will be used as my baselines. Monitoring will happen at frequent points throughout my treatment. Bone scans and CT scans will be done every 8 weeks for the first 6 months and every 3 months thereafter for as long as I am on the protocol. I’ll write more about the trial and the drugs (fulvestrant and GDC-0032) when I get underway on the 28th. I had a lot of trouble with with the blood portion as I only have my right hand and forearm for blood. It took six needles in that area (which included two blown veins) to get all of the radioactive tracers in and blood out. I will be discussing the option of putting in a port at my next appointment.
So the short story is that results were not as I’d have hoped. I wanted it to be clear that the cancer was still confined to my bones and lymph nodes, even if it were in more bony locations. This, however, is not what it seems to be.
First I need to explain about the tests. I’m going to briefly try to explain why it’s a bit of apples and oranges to compare my test from August with my tests last week and why all of it is a bit jumbled. In August I had a PET scan. In oversimplified terms this test picks up on high activity metabolic areas. So, cancerous tumors (and also some false positive areas on occasion) “light up” because they have a high number of rapidly dividing cells. It measures activity. CT tests, on the other hand, are static. They are like x-rays. They just take a picture without regard to whether the nodule/lump/tumor etc. is malignant. It shows there is something there but can’t necessarily tell you what it is in terms of metastatic breast cancer. CTs are very precise visually. PETs are not necessarily so. CTs in my case can’t tell us for sure if a spot is malignant.
I now have a small spot showing up on my liver that wasn’t visible on the PET in August. So is it a new metastasis? Or is it a benign spot that just didn’t show up on the PET because it’s not cancer? Who knows. We will have to wait and see if it changes when we do the next scans 8 weeks after the trial start (10 weeks from now). There are also nodules in my lungs and pleura. These are potentially (likely) malignant but the ones in my lungs have not changed size in 8 weeks.
I think that’s as much detail as I need to go into. The worst spots in my bones are my T12 vertebrae and my first rib/clavicle area. There are many spots but those are the ones that cause the most pain.
Unfortunately and most significantly at the moment, the scans also showed that the small pleural effusion (fluid in the lining around the lungs) has grown.
So we have many question marks with a few new areas of concern. For now we watch and wait. The pleural effusion will need to be drained if it grows or continues to cause breathing problems. For now any physical exertion gives me trouble. I need rest throughout the day but am trying to conserve energy for activities with the kids.
None of this news changes anything about my planned start of the clinical trial. Whatever these spots are and wherever the metastases are, the drugs I will start in ten days have the best chance to keep the spots stable and eventually perhaps shrink them. Reports from the phase 1 trial participants showed that often there was a stability period of about 8 weeks before some achieved some tumor shrinkage. I have ten more days to go chemo-free before I begin. I am counting the days. That start day is the most important day I have. A few of us in the trial are starting on that day so hopefully I will get to meet some of the other participants. There are 60 nationally in this phase 2 trial, approximately ten people will be at my location. There is relief in knowing there is no placebo in this trial. I may not respond but it won’t be because I received a placebo.
I wish I had better news about the scans but I also am resigned. This is what this disease does. I must do the best I can given my daily symptoms. There are questions marks and only time will give us answers. I try to have as much normalcy as I can, which often just feels like sleepwalking through the days and a bit of play-acting. But it’s important.
I keep coming back to a few lines I wrote recently:
Cellular biology is King.
But paired to that fateful ruler
I shall be an argumentative, rebellious Queen.
Wring the most out of each day.
Find those bits of joy and beauty,
Make sure that what I’m doing isn’t waiting around to die.
For truly, that would be a waste.
I can’t do anything more to change what’s happening inside. I have a plan and I just need the days to go by to get started. My quality of life is suffering at the moment but I hope that this will change. It is a rollercoaster, one I have been strapped inside unwillingly. Some days are good, some days are not. These happen to be some of the icky ones, but as always, I press onward.
Every morning I say to myself:
Find a bit of beauty in the world today. Share it. If you can’t find it, create it. Some days this may be tough to do. Persevere.
October 12th, 2013 §
 Hi all,
Hi all,
The interview on Al Jazeera America last night was not available to many who wanted to see it (even we don’t receive the channel). Thanks to my brother Mark I now have a link that you can use to watch it and/or download it. I am not sure how long it will be active so if you are reading this a few weeks or months from now I can’t guarantee they will still be active.
I think the show was great, I was so happy to be featured with Gayle Sulik and Dr. Susan Love… we definitely could have continued the coversation for another half hour. Kudos to AJA for giving us the time.
The photo above is of two of my nieces watching me on TV. Love it!
I welcome your feedback in the comment section. I wish I could have said more about metastatic disease but that wasn’t the true focus of the show.
Hope you all are enjoying your weekend.
October 7th, 2013 §
 There comes a moment in many conversations,
There comes a moment in many conversations,
I can see it:
They reach their limit.
Ten minutes in, or maybe only five,
They start to drift off,
Squirm,
Just want to be done with it.
Sometimes they even say,
“Let’s talk about something else” or
“Let’s change the subject”
Every so often they go as far as to say, “This is depressing.”
Being done with it is something I would love to do.
I’d love to tell the inner me to forget about it.
But that’s not possible.
It’s not mind over matter when that matter is making you sick, as are the treatments you need to fight it.
Metastatic cancer is background music, but it is a cacophonous roar.
I put it in its place,
But it has a place.
And the fact that it even has a place,
Well, that is just the way it is.
I try to keep its place as small as possible.
For as long as I can.
But I don’t have the luxury of changing the subject or forgetting about it for a while.
Like a greedy child metastatic cancer demands attention.
I tell it to wait,
Give me a bit of a break.
First I demand it.
Then, worried, I ask again contritely.
Then I downright beg.
Please, just give me some more time.
But I don’t believe there is anyone who hears me.
I don’t believe there is a god listening,
And I don’t believe cancer gives a damn about it all.
And so the plea evaporates as quickly as it came,
The tree in the forest with no one to hear.
I can only do my research, try to make the best decisions.
But in the end,
These cells will do what they will,
As they have,
Without respectful regard to all of my attempts to banish them.
That’s not how it works:
You can’t wish them away,
Hope them away,
Love and light them away.
Cellular biology is King.
But paired to that fateful ruler
I shall be an argumentative, rebellious Queen.
Wring the most out of each day.
Find those bits of joy and beauty,
Make sure that what I’m doing isn’t waiting around to die.
For truly, that would be a waste.
And in those conversations now I am grateful there can be other subjects to move on to,
Share the lives of my friends and support them,
Even if I am simultaneously pretending I can’t hear the roar.
The greedy child still tugs at my hem,
Will not be denied.
I needn’t let that noise drown us out,
And it won’t silence me just yet.
October 4th, 2013 §
 Once again Facebook games about breast cancer are making the rounds now that it is October. I posted this last year and got some flack from people who thought anything that “raised awareness” about breast cancer was good and couldn’t understand why I am critical of these messages.
Once again Facebook games about breast cancer are making the rounds now that it is October. I posted this last year and got some flack from people who thought anything that “raised awareness” about breast cancer was good and couldn’t understand why I am critical of these messages.
My point is that this isn’t awareness.
There probably isn’t anyone on Facebook who doesn’t know that breast cancer exists. But there certainly is a lot of myth-busting to be done. This is not how to do it. Topics that do need attention include male breast cancer, the underfunding of metastatic research (30% of people with breast cancer will eventually have metastases yet less than 5% of breast cancer funding overall goes to metastatic research), the fact that for many breast cancers 5 years in remission does not mean you’re free from risk of recurrence, not all breast cancer presents with a lump (inflammatory breast cancer)… the list goes on and on.
There’s a lot of work to be done educating. Education is awareness, these Facebook posts are not.
A friend asked me, “What can I do to help? I can’t donate money to your research fund but would like some ideas on things I could do instead.” What a great question. Rather than post these messages on your Facebook page here are a few easy ideas:
1. Make sure you are properly vaccinated from vaccine-preventable illnesses. This includes your family (kids and your parents if applicable), friends, and anyone else you can get involved (nag). Boosters like those for pertussis are very important. Get your annual flu shot. People over the age of 65 and some others at high risk should also talk to doctors about the pneumonia vaccine.
2. If eligible, donate blood and platelets. These products are needed by cancer patients constantly.
3. If eligible, get tested to be a bone marrow donor. Go to BeTheMatch.com to see the requirements. The initial registry just requires a cheek swab. It’s easy as can be.
4. Read blogs/follow tweets by people living with cancer. I think understanding the day to day lives of those of us living with it is a great way to truly become more aware. It’s one of the reasons I spend so much time writing here. I try to bring you the science, the experience, the thoughts of a mother trying to cope with raising a family and managing an terminal diagnosis.
Now on to the Facebook posts… here is a slightly modified version of the post from last year. You can go back to the original if you want to see comments made then.
……………………………
I don’t usually rant, but something has me steaming. Today the following exact message appeared in my Facebook inbox:
So here is the time of year again when we try to raise awareness for breast cancer through a game. It’s very easy and I would like all of you to participate. Two years ago we had to write the color of our underwear on our wall. Men wondered for days at what was going on with random colors on our walls. This year we make references to your love life status. Do not answer to this message just post the corresponding word on your wall AND send this message privately to all the girls in your contact list!!!!!! BLUEBERRY = single; PINEAPPLE = it’s complicated; RASPBERRY = I can’t / don’t want to commit; APPLE= engaged; CHERRY= in a relationship; BANANA=married; AVOCADO= I’m the better half; STRAWBERRY= can’t find Mr. Right; LEMON = want to be single RAISIN = want to get married to my partner. Last time the underwear game was mentioned on tv, let’s see if we get there with this one !!!!!Copy and paste this message into a new one and send to all your girly friends and update your status with your answer. DO NOT RESPOND TO THIS CONVO, just leave and participate.
One version I received yesterday says this:
Hello Ladies, Without replying to this message, put a heart on your wall; no comment, just a heart. Next, post a heart on the wall of the person who sent you this message. Then send this message to your women friends, only women. If anyone asks you why you have so many hearts on your wall, don’t tell them. This is only for women, because this is breast cancer research week. One small act of solidarity between women. PS to type a heart, first type < then 3 It will turn into a heart as soon as you post.
………………………
I’m going to keep my reaction short. I’m hoping writing something down like this will allow people who are as infuriated as I am with these silly requests to have something to react with.
First, I give you permission to ignore this crap. Better yet, write back to the people who have shared it. Let’s do some real awareness here.
The above instructions are not awareness. This is offensive. Breast cancer is not a joke, awareness does not come from sharing the color of your underwear or your marital status (the whole “tee-hee, wink-wink” attitude adds to my disgust). Even if it ended up on TV, that still would not be educating people about breast cancer they didn’t know before. All it does is show the world that lots of people are willing to post silly things as their status updates.
Let’s do a piece of education right here. The status update says “only send this to your girly friends.” Men get breast cancer too. Men are also the husbands, fathers, sons, brothers, and some of the friends, coworkers, nurses, and doctors who care for and are left grieving for people (men and women) who die of breast cancer. We should not exclude them from ANY discussion of cancer.
Just because it says it’s about breast cancer awareness doesn’t mean you have to agree. Go ahead. Ignore it. Or write back and tell them why you don’t want to be included in these things anymore. Another blogger, Susan Niebur, wrote about her take here. She was an astrophysicist, by the way. She died of metastatic breast cancer.
Anyone who has breast cancer and uses your FB status update as an indicator of whether you support their cause is not very enlightened. When I rank “how to help those of us with cancer,” sharing one of these paragraphs as a status update is the lowest possible method of showing support. There are endless ways to do that. I think it actually is the opposite; sharing these status updates makes people feel they are doing something real for breast cancer causes when they aren’t.
I’ve also had it with the I’ll bet most of my friends won’t share this post attempt to guilt me in to sharing something like “share this if you think domestic abuse is awful.” “Share this if you think autistic kids are special.” Well yes, actually, I believe both of those things. And just because I didn’t share them as my status update doesn’t mean I do NOT agree with the statements.
Education underlies awareness. To even call something a game and honestly believe it’s doing anything to help any aspect of this disease is delusional.
And why would awareness be correlated with something being done secretly?
I think that those of us who have had breast cancer have an obligation to speak out if we disagree with these posts. People look to us to see how we react. If we not only read these updates but share them, it does constitute endorsement. It says we agree. It says it’s okay to think of breast cancer awareness this way.
I say: count me out of these Facebook games.
I have stage 4 breast cancer and it is no game to me.
October 1st, 2013 §
 This is the last photo I took before I found out I have metastatic breast cancer.
This is the last photo I took before I found out I have metastatic breast cancer.
This photo was taken in the final days of September when I went to visit my surgical oncologist for my annual checkup.
I’m wearing a hospital gown with those boots. The contrast of the gown and boots made me laugh.
I snapped the photo.
The actual diagnosis came one year ago today.
It came on the first day of Breast Cancer Awareness Month (a month which has always driven me batty).
It came more than five years after I finished treatment for stage II breast cancer (no, five years without a recurrence does not mean you’re cured, let’s just bust that myth right now. Hormone receptor positive breast cancer in particular can return after 5, 10, 15 years or more).
……
I went to my surgical oncologist annually so she could check on how I was doing after she surgically removed both breasts in January of 2007. After the active post-surgery period, the visits consisted mainly of a physical exam and a talk about how I was doing and what post-chemo treatments I was on.
At this particular visit I complained of some rib pain in a place where I’d broken two ribs in a fall a few years prior. Nothing else was bothering me that day. While I was changing into my street clothes she phoned downstairs to my medical oncologist who said he would put orders in to repeat my bloodwork a month early. It was a test he did every six months at that point.
None of us were worried.
Flash forward a few days to Monday, October 1, 2012.
One of my medical oncologists (I have two, one is a general hematologist/oncologist and one is a breast oncologist) walks into the room with a concerned look on his face and says hello and goes straight to the computer. He starts punching things in to log into the system.
I ask him, “How are you?” “Not so good,” he says. I am sure he’s talking about himself, his family, his favorite sports team perhaps.
“Your markers are elevated,” he says. And only then does he turn to make eye contact with me. I know now, looking back on it, it was too hard from him to tell me. He really didn’t want to deliver that news that day.
When he tells me, he knows I know what that means. We’ve been a team for more than five years by then. He knows I know. It doesn’t need to be explained.
He looks at me while I crumble. And swear. A lot. He comes over to comfort me. I am alone in that room with him. No one expected this to be anything but routine. I didn’t bring anyone with me for the appointment, I almost never had company with me at any of my appointments over the years. That’s how I liked it most of the time. I still do, actually.
But today’s visit rapidly becomes the farthest thing from routine.
……
I wasn’t expecting it. I confess that. The pain I’d complained about a few times during those five years? That pain had never turned out to be anything.
And oh… by the way, that rib pain that I complained about? It actually was nothing. It was just sore ribs from the old fractures.
I was sent across the street to the hospital immediately for a chest x-ray. This looked clear. My PET scan the next day showed no cancer where I’d complained of soreness. But there was cancer elsewhere: in multiple bones and lymph nodes. It really was what we feared. We were lost, falling, reeling, grieving.
Within three days I was having a surgical biopsy through my neck to gather malignant tissue and lymph nodes. Within two weeks of the news I had the true sign that would have taken me to a doctor anyway: bone pain in my collarbone area from a fractured first rib caused by cancer breaking through the marrow into the bone.
I’d have found out within a few weeks that I had metastatic cancer anyway when the pain in my shoulder got severe… which is why some doctors don’t even use tumor marker tests. The marker tests don’t reflect cancer activity for everyone. Physical symptoms are usually quite reliable. And let me also point out that a lot of muscular pain can be hard to distinguish from bone pain depending on location. I’ve had both. And it’s not easy to tell them apart in my opinion.
I went and met with my other oncologist a few days after that.
I started chemo within ten days of hearing my diagnosis.
Things moved fast.
Life changed forever.
……
The weather is changing now. It’s warm this week so I don’t think I’ll be reaching for those boots.
But when the cool air comes again in a week or two or more I am not sure how I will feel when I reach for them.
Right now they just make me feel sick.
September 30th, 2013 §
 Here we are again. A crossroads.
Here we are again. A crossroads.
The third of many we will have.
I’ll give a bit of a recap. I know it gets quite technical but documenting the details is important for those who also have metastatic breast cancer.
It’s almost one year to the day that I was diagnosed with metastatic breast cancer in my bones and lymph nodes. I started on the cytotoxic daily drug Xeloda first (in addition to monthly infusions of Zometa) which gave me six months of success, shrinking the amount of cancer evident on PET scans.
In April 2013 when my tumor markers started rising I started on the hormonal combo of Aromasin and Afinitor (and also switched from Zometa to Xgeva because of difficult side effects I was having). I started on a 5 mg/day dose of Afinitor with a 25 mg dose of the Aromasin. I gradually increased the Afinitor dose to 7.5 mg/day, and then when my markers began to rise again a few weeks ago, I started on 10 mg a day.
It has now been five months on this combo (in all of its different dose strengths) and my markers are rising. This chemo is no longer working. So, it’s time to decide what to do next.
Regular readers will know that this is typical of metastatic breast cancer: some therapies may not work at all while some will work for a while. Ultimately, though, the cancer becomes resistant to each of these treatments and will progress. Sometimes you get a great response and can reduce the amount of cancer that is present. Oftentimes you settle for the success of “stability” where the cancer isn’t reduced, but it also isn’t growing. It’s often referred to as hanging out with “Stable Mable.” This is still a good response in most people’s books.
Especially when your cancer is still confined to your bones and lymph nodes, stability has the added feature of being life-saving: as long as the cancer is in those places it cannot kill you. Only once it metastasizes to organs can breast cancer kill.
So… now it’s time to decide what to try next (this part gets technical). Right now it’s looking like I’m headed to a clinical trial of a drug that has shown promise in breaking the resistance of hormone sensitive breast cancers especially in people like me whose cancer displays a Pi3k mutation (40% of people with ER+ breast cancer have one of these mutations). This experimental drug would be in combination with a drug commonly used for my kind of cancer (Faslodex). I’ve enrolled with the clinical trial team. This is a Phase II trial so I would be guaranteed to get the experimental drug.
What does this mean? In simple English, it means I’m trying a new drug that’s designed to break the resistance of this particular kind of cancer to treatment. It seems to be especially effective for those with the type of cancer mutation that I have (Pi3k-alpha). If this drug makes the cancer susceptible to therapy, then the other drug I’m taking can do its work. This class of drugs is at the forefront of where cancer research trials are right now.
I’ve been pre-screeened and have a few more hurdles to clear: scans, bloodwork, and a three week “washout” period where I must be chemo-free to allow any residual effects of my current treatment to clear. Am I nervous about a period with no safety net? Yes, a bit. But I also am curious how my body will react to having current chemo clear my system. I’ve had a lot of trouble with things like high blood pressure, high cholesterol, rapid heart rate, shortness of breath, and headaches in the past few months. I’m interested to see how many of these will improve.
The new drugs will have their own series of side effects, some of them might be similar and a few may be different and more serious. So this three week period sits okay with me because if my current treatment isn’t doing anything anymore, it’s of no use anyway.
There will be so much to share about being involved in a clinical trial. And I will share that with you, should I make it through the final screening process. I am learning so much as I go and I think there is a real chance here to inform others about the experience. Trials are as varied as can be. Each has criteria that must be met. Sometimes you end up on the good side of these and sometimes you don’t.
My oncologist looked at a host of trials before we chose this one. I was ineligible for many of them because of the drugs I have already tried, my particular features of my cancer, what cities the trials were offered in, when they were enrolling patients, etc. Some were not attractive to me because of the phase of trial that it was (I’ll explain in a separate post the differences between Phase 1, 2 and 3 trials). I am glad to be in a trial where a drug has already passed initial safety standards and will also be given to every patient in the group (there are no placebos in this phase of trial).
It’s important to note that a clinical trial should not necessarily be viewed as a “Hail Mary” meaning it’s the last remaining hope. In reality, my sense is that this is very rarely the case, at least with Phase 2 or 3 trials. They can only establish true efficacy in people who are still at certain phases of the disease process and haven’t had too many chemotherapy agents already.
To me the key was to find a trial that had a good scientific basis for success, was currently enrolling patients and was within commuting distance. In addition, I think it’s best if the standard of care drug is one you would already be considering using at this point in your treatment. There is a database at www.clinicaltrials.gov where you can search for trials.
I have reserved my spot in this trial. If I meet the testing criteria I will be one of 60 patients nationwide on this particular protocol, about 10 at my particular location. I view it as an opportunity. It is well-suited for my cancer at this time in treatment. It’s using the newest thinking in targeted therapy based on genomic analysis.
It’s scary, yes. But if it doesn’t work I still have standby treatments to go to (and other trials by that time that I hopefully would be eligible for). I know there is no cure. But maybe this one will give me a chunk of time.
I won’t go into details here but I know people will ask what’s involved. The treatments will be injections (Faslodex is two big intramuscular injections in the butt every month after doses every 2 weeks the first month) combined with daily oral capsule (the experimental drug). I will also continue to get an Xgeva injection in the arm each month. There will be a strict schedule of fasting bloodwork in NYC every two weeks and scans every 8 weeks to monitor the cancer’s growth. I’ll have to keep a medication diary. I’ll let you know how everything else works once I am underway. It’s a lot of work, especially in the first two months including all of the meetings and tests just to get started.
There are so many questions I know people will have. If you post your questions in the comments I will do my best to answer them in future posts if I can. You may post them anonymously if you like. For now I’m not going to state the name of the drug (actually just a string of letters and numbers) until I’m actually enrolled.
It was quite devastating to get the news that the current chemo isn’t working anymore. It always feels like the rug being pulled out from under me. I always cry. I always feel like I’m falling.
But plans are my safety net. Options are my lifejackets.
I leap from treatment to treatment on my tippy toes, knowing if I place too much weight I will sink.
This is the dance I do now. Forever.
September 29th, 2013 §
 With great sadness I announce that Jen Smith, featured in an interview here less than a month ago, died yesterday (September 28, 2013) at the age of 36 from metastatic breast cancer.
With great sadness I announce that Jen Smith, featured in an interview here less than a month ago, died yesterday (September 28, 2013) at the age of 36 from metastatic breast cancer.
Readers who receive these posts by email may not have had a working video link to see a 2 minute video of Jen and her son that was included with that interview. I am including a link to my original post here so you can either read the post if you missed it, re-read it, or just go to watch the video which appears at the bottom. I promise it is worth two minutes of your time. It makes me smile and cry in equal measure every time I watch it. It also tells the story of how Jen found the tagline “Live Legendary.”
The obituary the family posted appears here and you can read how much Jen accomplished in her too-short life. I wish I had known her longer; I am jealous of her friends and family who did.
Over the past few weeks we texted. Some days I just texted her to tell her I was thinking of her. Some days I would get a reply as to how she was doing. Some days I received no reply. Those were hard days as I worried so much about her, knowing she was about to die. I continued to text her almost daily in the last two weeks even when there was no response. My last text to her said, in part, “I cannot help myself from saying I love you for as many days as you are here to hear it.” When you have stage IV breast cancer you bond quickly with others who have it too. I do not know if she read that message.
Jen and I spent the last few months having very serious conversations about life and death. I wish we could have been two friends talking about other topics instead. But I am gratified that we could talk openly about some of the things were on her mind the most as she reached the end of her life.
My condolences to her friends and family including the light of her life, her sweet son, Corbin.
September 23rd, 2013 §
 It takes a leap of faith every day.
It takes a leap of faith every day.
Not one of religion– no that’s not in my play book.
But there is a leap that comes when you think to yourself each night,
“The world will be here tomorrow, and I in it.”
Statistically it is likely to be so.
But what about the day after, and the day after that?
How many days do you think ahead?
Have you bought plane tickets for next year?
Planted bulbs for Spring?
Bought an extended warranty on the washing machine?
Three years ago, without even a thought, I took a three year car lease.
Nine months later I received my diagnosis of metastatic breast cancer.
Fifteen months from now that lease will come due.
Will I take another?
I have a car in mind I would love to have…
But can I think of my life in fifteen months,
What it will be,
What will I be?
No, I cannot.
I talk of taking trips in Spring. I have a friend down South I want to visit.
I do believe I will be alive.
But what will my quality of life be?
What chemo or radiation or surgeries will I need by then?
What regimen will I be on and how will I feel from it?
Just being alive is not always enough.
I don’t buy those tickets,
But I do still think the thoughts.
I don’t make promises because I don’t want to cancel.
I say, “Let’s play it by ear,”
“Let’s see how it goes,”
Because to plan, to get hopes up,
To think it could come true…
And then to have them dashed
Would be too hard for me.
I know not everyone shares this view.
The thing with incurable cancer is I don’t have a particular kind of hope anymore:
I can’t have the confidence the suffering will end because it is temporary.
It is not temporary.
I do keep pressing forward though, in my own way:
With strength, with dignity, and yes, still with great hope for more time.
Many days that is one of the hardest things about it all:
I can’t just mark the time and get through
Knowing the hardest parts will soon be over.
Because I know the hardest parts are yet to come.
September 19th, 2013 §
 I’m not about to let myself go.
I’m not about to let myself go.
I’m not about to stop wearing makeup or dressing nicely or styling my hair each day.
I’m not about to relax my standards or let my children get away with things they shouldn’t.
I’m not about to stop being a friend, a daughter, a mother.
I’m not about to stop having dreams.
I’m not about to stop learning, growing.
I’m not about to stop sharing.
I can’t just give up.
I can’t stop moving.
I can’t change who I am.
I know some of these things will change.
I know someday soon I won’t have choices about what I do each day.
I know there will be a day I won’t have hair to style again.
I push myself too hard each day.
I feel I am in a race against a clock.
I must pack as much into each day as I can.
I am in constant motion,
Like a summer child waving her arms to keep the mosquitoes away…
I dance and thrash and run away,
Looking for a place to escape injury where there is none.
I can’t control so many things about having metastatic cancer.
This feeling is one of the hardest things about this disease.
But those things I still can?
I’m holding on tightly onto those,
And I’m not about to let go now.
September 13th, 2013 §
 It’s always right when they pull the bar down over my head and jam it into my lap on the rollercoaster that I silently start screaming, “Wait! I changed my mind! Let me off!”
It’s always right when they pull the bar down over my head and jam it into my lap on the rollercoaster that I silently start screaming, “Wait! I changed my mind! Let me off!”
By then, however, it’s too late.
With a jerk the car moves forward, its underbelly grabbing the hooks to lift it skyward.
By the time we are moving, climbing, the car is making a clicking sound and I am sure this was a mistake. I wedge my knees against the back of the seat in front of me to minimize my movement.
I steel myself, knowing the drop will come whether I like it or not.
And then there is that moment, that nauseating violent moment before the floating…
For a brief portion of a second I’m airborne, held in by that suffocating bar. Down we go and I slam back into the seat. I tell myself it will be over soon. I just need to ride it out. It will end.
These days I’m on a roller coaster ride that doesn’t end — well, not anywhere good, anyway.
When we last met here for an update, I said the increased dose of chemo had shown a response. That response is proving to be short-lived. Yesterday my tumor markers were up again, back in the range where we need to discuss changing chemo again. It’s been about four and a half months on this chemo combination of Aromasin and Afinitor (I continue with monthly Xgeva injections).
This is the cycle of metastatic breast cancer: chemos inevitably fail. The cancer becomes resistant, mutates, signals a new pathway to drive its survival. We have no way to know how long each will last. When you read studies and “success” is deemed an extra two months of progression-free survival you know you’re dealing with heavy realities.
The immediate plan is to increase the Afinitor one more time, to the maximum. I’m told no one tolerates this dose regimen for long because of the side effects. But I’m almost at that dose now anyway, so let’s give that a go. Even if I can get a response for one month, that will allow me time to figure out what will come next. The two options are to continue with a targeted, anti-hormonal therapy of some kind or begin IV chemo after having a port put in. There are pros and cons to each, I won’t go into them here. Once I’ve made a choice I’ll fully explain it, of course.
And so, for now, I increase the dose. I wait. I retest again one week from now, and two. By then we’ll have a plan, and likely be moving on. Another tally mark of treatments tried to buy me time.
It’s too soon:
I fear the safety bar is not locked.
I fear that each time I reach the top of the hill again I’ll be ejected from the ride, skyward, only to plummet to the ground.
……….
Two housekeeping notes:
1. If you only want to read updates on my chemo status and current health, I make it easy for you by titling these posts “Update” + the date as the title.
2. I’m pleased to report that this website is now optimized for mobile device reading. If you read the posts on your smartphone or tablet you will note that you no longer have to scroll left and right to read; the posts are nicely contained in columns. There is a menu at the top to navigate the site and a clean layout. To comment on posts on your device, look at the end of each post for the “replies” link to click. This should make it easier for those of you on the go to leave a comment.
September 5th, 2013 §
 I don’t remember exactly when Jen Smith (@sinclair319) and I first connected on Twitter but we definitely hit it off: two straight-talkers with metastatic breast cancer, both determined to do what we could to live as long as we could while educating others about the day-to-day reality of living and parenting with a stage 4 diagnosis. Jen had already been doing it for years, and I have always appreciated the guidance she gave when I was diagnosed with metastatic breast cancer in 2012.
I don’t remember exactly when Jen Smith (@sinclair319) and I first connected on Twitter but we definitely hit it off: two straight-talkers with metastatic breast cancer, both determined to do what we could to live as long as we could while educating others about the day-to-day reality of living and parenting with a stage 4 diagnosis. Jen had already been doing it for years, and I have always appreciated the guidance she gave when I was diagnosed with metastatic breast cancer in 2012.
Jen and I are direct about our shared goals (she has a son, Corbin, who is 6. He’s about the cutest boy you will ever see. The photo above was taken a few months ago). Some of our goals: be honest about cancer with our children in an age-appropriate way, be public about the reality of parenting with incurable cancer, teach independence and joy to our children and let them know these are important to experience even after we are gone, and finally, to live life to the fullest even while undergoing difficult and often debilitating treatments for the rest of our lives.
Jen was diagnosed with at age 30. I encourage you to visit her website www.livinglegendary.org to learn more about her story and her writing (her two books are titled Learning to Live Legendary and What You Might Not Know: My Life as a Stage IV Cancer Patient).
The sad reality of metastatic breast cancer is that it kills. In fact, it’s the only kind of breast cancer that can kill.
Jen is now dying. She has entered hospice after being told in late July that no other treatment options were available.
I have few ways to help Jen in her remaining time alive but one way I thought about helping her was to share her story and her spirit with my readers. I asked Jen to answer some questions for me about two weeks ago and she graciously accepted. I know that today she would not be able to spend the time and energy doing this, so I really treasure the words that she has written.
………….
Lisa: First, I want to refer to a line in your book What You Might Not Know. You write that when your friend Erin was dying you panicked. You asked, “Would others feel this same panic when I was dying?”
I would like to tell you that right now, in this moment, the answer is yes. We feel the panic. I feel it acutely. And the helplessness.
Jen: The difference was Erin just had palliative surgery to alleviate her neck pain. She was supposed to heal from that, then go on for more treatment. But, during recovery at home, she became short of breath, begged her mom to call 911. By the time they got her to the hospital, they were able to keep her sedated until her husband flew in.
I’ve watched many friends die, and the “shocking” ones like this one (and the one who just went to have a blood transfusion, then had a clot thrown in her lung and kill her) often offer a different kind of grief compared to those who go on hospice and you have “warning” that their life is coming to an end. You can brace for the looming grief.
Lisa: As an introduction, can you please tell readers what your current health is today (August 17, 2013) and why you have entered hospice. Are you currently receiving any treatment? Do you receive palliative care? Most people think of hospice as something for the last week or two of life. If you would, please share what hospice will provide for you now and going forward as you move closer to death. Do you encourage people to get involved with them sooner rather than later?
Jen: After nearly 6 years of treatment for breast cancer, on July 31st, 2013, my doctor said, “I’m sorry, we’re out of options and it’s time to refer you to hospice.”
I’ve watched a lot of friends die from this vile disease. I’ve always thought, “When hospice gets involved, I hope I go quick, in a matter of hours or days.” Now, after being on hospice for over 2 weeks, I have a different perspective. Hospice is all about comfort care…what can be done to make the patient more comfortable? While on hospice you are not allowed to receive any treatment that would be considered actively trying to kill the cancer cells (i.e., chemo). But, hospice often goes hand-in-hand with palliative care which is about relieving the pain and stress from a serious illness.
I have drains in my lungs which drain out the fluid which has built up due to the amount of cancer present. This is palliative care. It isn’t going to stop the cancer from progressing, but it is going to enable to breathe easier. When my lungs are full of fluid (sometimes close to a liter per side) my oxygen intake is pretty minimal. Because of this, my heart has to work harder to pump out that oxygen to my body. With my heart working so hard, my whole body is tired. Being able to drain my lungs takes care of the shortness of breath issue and also gives me a bit more energy since my heart isn’t working as hard.
Right now I meet with hospice weekly. I got to decide the frequency. I’m still fairly independent; I’m not confined to my house or bed. As the disease progresses, I expect that I will meet with hospice more often. Although they only visit once a week, I speak with them almost daily. They are in charge of reordering any of my supplies (i.e. lung drain kits) and refills of medication. It’s great being able to call, tell them what you need, then it magically shows up at my front door. Hospice is like a good friend, not the enemy. I’d highly encourage readers to consider their services as soon as necessary.
In full disclosure, my mom has taken FMLA time and is staying with us (I’m a single mom to a 6 1/2 year old boy). While I’m still independent, I’m able to be that way because my mom is helping with all the behind the scenes stuff. Laundry, groceries, cooking, cleaning, etc. This way I’m able to conserve my energy and use it with my son.
Lisa: You have a beautiful son, Corbin, who is about to start 1st grade. I know when you were first diagnosed with cancer at age 30 and then with metastatic cancer only 3 months after completing your original chemotherapy you set a goal of living to see him enter kindergarten. What does the advent of school mean for you emotionally now that the first goal was achieved?
Jen: Correct, I made the goal of seeing him start kindergarten when he was almost 2. I knew the statistics were against this, but it also gave me a very concrete goal. Of course I had short-term goals along the way, but this was always the ultimate goal.
Last year when I took him to his first day of kindergarten, I was excited, thrilled, and so very thankful that I got to watch him walk in the front doors. This year will be different emotionally.
In early August we learned who his teacher was. We learned his best friend would be in his class in addition to many of his friends from kindergarten. My son, like many his age, thrives on consistency and structure. I am divorced and his father lives in a town about 20 minutes away.
When I was referred to hospice, I decided that I would start my son at the school in his father’s district. I figured it was one less transition he would go through at the time of my death. So next week, when I take him to his first day at his new school, it will be a mixture of emotion. I’m so grateful that I’m able to see him start another year, yet heartbroken that him starting this school will be the first of many, many changes for him.
Lisa: How has your relationship with your physicians changed throughout the last six years with metastatic disease? And now that you have been told you are at the end of your life?
Jen: I’ve had the same primary oncologist who has always been in favor of 2nd opinions. I joke that I’ve become a hospital hussy going for 2nd, 3rd, 4th and even 5th opinions. But, my primary oncologist has always been my “go-to” person. My oncologist has been in practice for 25+ years, so he is good at keeping the doctor/patient relationship boundary, but I’m willing to bet I’ll stick out in his mind, even after I’m gone.
Lisa: What are you are most proud of accomplishing?
Jen: Memories with my son, family, and close friends. The walls of my home are covered with pictures from different vacations, photo shoots, and events. I’m not interested in fine art, I’d rather have those pictures, and those memories adorning my walls instead.
Lisa: What do you want to be your legacy above all, besides Corbin, of course?
Jen: I feel like this is a trick question-ha! My legacy…wow, that’s a big one. I think the biggest thing is I would want people to stop being the victim in their own lives. I’ve met so many people who have the attitude that they are the victim, everyone is out to get them.
I guess I would want my legacy to be for those people to take responsibility and control what they can. Don’t get me wrong, bad things happen to good people…and I’ll NEVER say “cancer is a gift.” It is not. It’s a thief and a murderer, not a gift.
But I’ve used having cancer as an opportunity to do some things in my life that I may never have done (leave my job, take a huge cut in pay, but go with the mindset of being on retirement and do things retired people do, i.e., travel!)
Lisa: I know you are a believer (as I am) in writing your own obituary so that certain words or phrases commonly used in describing the death of someone from cancer would be omitted. What did you feel it was most important to include and what language did you specifically want to avoid?
Jen: Language to avoid: “lost her battle” “was an inspiration and fought” “cancer was a gift”
Mostly though, I wrote my obituary and planned most of my funeral because I saw it as a gift I could give my family. At the time of my passing, when they are numb and filled with grief, I didn’t want them to have to try and remember what awards I’d won, what year I graduated high school, or when I started at a certain job. I saw this as a gift that I could provide them.
Lisa: What song do you feel best describes your life or your outlook?
Jen: I’m stuck on this one…not sure that one describes my life or outlook. There are ones that I want played at my funeral for specific reasons/to bring comfort during that time.
Lisa: You and I have many similar approaches to dealing with our cancers. We were diagnosed originally at a similar time and when we each had a child under one year old (I also had a 3 year old and 7 year old at the time). One thing we differ greatly in, however, is religion. You write in your book that you think God has a plan for you and that you believe in Heaven and seeing others after you die. You write that you “could not have gotten through this” without your faith. As an atheist who believes this life is all there is and never prays for nor believes in miracles, I am wondering if/how your religious beliefs have changed as you have come closer to death.
Jen: I’ve witnessed a miracle and I see him every day. I’ve been more forthcoming in sharing the excruciating infertility experience I went through to get pregnant. There is no way the last cycle should have worked. There were too many variables that were not in our favor. But, a miracle happened, and Corbin is living proof of it.
I was raised Methodist and still attend the same church I attended as a child. While I go to church regularly, I don’t consider myself “religious” because I can’t quote Bible verses/stories. I consider myself as having a “strong faith.” I’ve witnessed too many completely amazing things to believe they were mere coincidences. I’ve met people (on mission trips) who are so financially poor that they live in trailer and use an outhouse, yet they are so rich in life.
I see Heaven as a huge “welcome home” party. I remember reading a quote that says: One day God says, “Enough, come home.” And that felt so comforting. I know that I’ll be reunited with family members, friends who were stolen from this disease, and most importantly, the child I carried but never met on Earth. And, I think that in terms of eternity my family/friends/son will join me in the blink of an eye. My faith, which Corbin has learned has brought great relief during this time. He knows that he will see me again and that I’ll be waiting for him at his “welcome home party.”
Lisa: Are there any decisions about your treatment in the past six years that you regret? That you think were not fully explained? I, for example, had an oophorectomy (as you did, too) but feel the side effects and long term health risks of having that surgery (increased risk of lung cancer, for example) were not fully explained. And, on the flip side are there any treatments you feel were particularly important in extending your life?
Jen: I can’t think of any.
Lisa: What are a few things you think are the most important myths we should debunk right here, right now, about metastatic disease?
Jen: I know society and the media have conditioned us to use the language “battle” against cancer, or in the “fight/war” against cancer. This is something that I’ve never really felt connected to. After all, what am I battling? A rogue cell in my own body, so in essence, I’m fighting myself. The best quote I’ve found that relates to how I feel is when Elizabeth Edwards died in 2010. Her friend said, “Elizabeth did not want people to say she lost her battle with cancer. The battle was about living a good life and that she won.”
The other frustrating thing I run in to is “So-and-so tried XYZ therapy and was stable for 10 years, why haven’t you done that one?” Then I explain that I tried XYZ and had progression in 3 months. I think getting people to truly understand that this is such an individualized disease is key. Just because XYZ works for one person doesn’t mean all people will respond the same way.
And, this is just me, personally, but I hate being referred to as “sick.” I’m not sick; I have a disease called metastatic breast cancer. If I was “sick” that would imply that I’m possibly contagious or that I’ll get better, neither of which are true.
Lisa: Your son has never known a time in his life when you didn’t have cancer. He is very astute and caring and sensitive. He is a joyful boy is not afraid of many of the topics and subjects that many parents try to “shield” their children from.
I know you and I both believe that protecting children by withholding information is not the right thing to do. Age-appropriate information dispensed in small pieces is better. Do you notice that other parents are uncomfortable around you and Corbin for this reason?
Jen: Maybe I’m completely naïve, but I haven’t noticed that other parents are uncomfortable around Corbin and me. More often than not, I’m told, “Thank you for being so open. My aunt/grandma/relative had cancer but we really didn’t know about it until she passed.”
I’ve worked to connect with as many as possible and be as transparent with information as possible. People assume that a bilateral mastectomy means a “great boob job” at the end. I’ve posted pictures of my bilateral mastectomy (without reconstruction) to educate others. I’ve also posted a picture of my scan, so when I say “it’s everywhere” they can see the scan that shows it truly is everywhere. This was an especially powerful message because I look so “healthy” on the outside.
Lisa: I’d like to leave readers with your video which is one of the most beautiful tributes to a loving relationship I’ve seen. I implore readers to spend two minutes of your life seeing Jen and Corbin. They will make you cry and make you smile. If there is anyone who knows how to live legendary, it’s Jen.
Jen, thank you for sharing your precious time with me, and with so many others. I promise you that your enthusiasm for life and your powerful message will live on in the hearts and minds of so many. It is an honor to call you a friend.
August 29th, 2013 §
 Remember me pretty,
Remember me pretty,
Remember me whole.
Remember me the way I am today
While friends still honestly say, “You’d never know.”
Let me tell you:
It’s not what it looks like,
It’s not what it seems.
Those times are long over,
Now I am on my own.
The beggars have all ridden.
My wishes: horses gone.
I float above it all,
Watching as I do.
Surrounded by people,
Feeling so alone.
Head down,
At the stoplight tears come,
A young man pulls up next to me
Glances once… twice…
With an engine rev, he’s gone.
I hide it pretty well, you see.
They say, “You look so good,”
“You are so strong,”
But in the space that’s in between
I fall apart
I kick and scream
I claw and grab on for dear life.
Because really,
Truly,
What is happening here:
Choice is gone,
Chance is Queen,
Luck will run right out.
Everyone placed their bets?
Let’s see how far we can go.
August 24th, 2013 §
I had my PET scan on Thursday morning and received the results yesterday. I suppose the best way to simply summarize it is that it’s a mixed bag.
There is mild progression from my scan in April. This means there are more sites of cancer in my bones that are large enough to be detected on these scans (“hot spots”). One hip, one side of my pelvis, one thigh, more tissue and some nodes in my upper chest are all newly affected. Many ribs and one vertebrae continue to be pretty plagued as well but were already lighting up on previous scans.
That said, it is good news that the metastases are still confined to my bones and nodes (honestly, I can’t believe the things I call “good news” these days!). There is no evidence on the scan that it has spread yet to my liver or lungs.
So the scan is overall worse than April but still better than October in that the spots are in the marrow and not eroding bone itself (the fracture I had in my collarbone has healed and the cancer diminished there). This is good and also has the benefit of keeping me mostly pain-free. My chemo causes muscle inflammation which hurts but it’s surely preferable to bone pain. Most other side effects have been the same as before.
So here is where it gets tricky. And if you haven’t figured it out by now, this whole business is quite complicated and full of guesswork. My tumor markers had been rising and it looked like we would need to move to a different chemo. At that point (about a month ago), we decided to increase my chemo dose and see if we could get a response. After two weeks my markers dropped. That was right before the scan.
So, one takeaway is that we are learning that my bloodwork is quite accurately reflecting the cancer’s response to chemo. This is not the case for everyone.
So the million dollar question is: is the scan reflecting the peak progression this time and now that I am on a higher dose of chemo if I continue to have lower markers will we see the scan reflect this in another few months? That is, is the scan showing the worst it got and now with the recent increase in chemo it is actually on a downward trend? That’s the hope: continue to see response. Only time will tell where on that dynamic process this static measure is.
This information puts me in limbo yet again. But that’s really what this world of metastatic breast cancer is. And you know, I would rather have limbo than definite bad news (again, I chuckle at the straws I grasp at here…).
I won’t go into details because this post is growing long, but I did meet this week to discuss possibly enrolling in a clinical trial at Sloan Kettering. This would be a phase 1 trial and would be a strict chemo protocol. I will do a separate post about trials in the future because I think there is a lot to learn about them and also a lot of misinformation about their use with this disease. Bottom line on this particular trial: it wasn’t one I would definitely jump to enroll in. Some additional time to explore it and other options some more would be nice. So “limboland” helps with that, too.
For the next few days (and likely the next few weeks) I will continue taking the higher dose of chemo daily, monitoring the bloodwork every two weeks. I’m having shortness of breath for the first time this week and that is quite unpleasant. It is a side effect of the chemo.
The results are not what I hoped for. But onward I go.
I deal with what is, I adjust to new information as quickly as I can and forge ahead into the unknown.
I thank you for your care and concern this week. As always, it takes some time for me to gather, interpret, and process the information before coherently getting it out to you all.
August 20th, 2013 §
This is the last week of summer before school begins.
 This summer was a big one for us. Youngest Tristan went off to sleepaway camp for one week and loved it so much that in the end, he stayed for a month. Paige and Colin returned to camp as seasoned veterans and had a wonderful time in their home away from home. All learned new skills and made new friends. Paige and Colin’s constant banter of camp stories at the dinner table are now supplemented by Tristan’s own stories.
This summer was a big one for us. Youngest Tristan went off to sleepaway camp for one week and loved it so much that in the end, he stayed for a month. Paige and Colin returned to camp as seasoned veterans and had a wonderful time in their home away from home. All learned new skills and made new friends. Paige and Colin’s constant banter of camp stories at the dinner table are now supplemented by Tristan’s own stories.
I’m so pleased they could be in a place where they could just be kids, not worried about me, free to be carefree and happy. It is my gift to let them go, to not keep them here for my own needs. While I want to spend as much time with them as I can, I know that this is what they all needed to do this year.
 I sit back and smile now, loving that they all have a common reference point of their weeks at camp. Despite the eight year age gap they all find laughs and joy in their summer adventures. They look older to me, of course. And while others are sad about the passage of time and their children growing older and being independent, I say again that I cheer it.
I sit back and smile now, loving that they all have a common reference point of their weeks at camp. Despite the eight year age gap they all find laughs and joy in their summer adventures. They look older to me, of course. And while others are sad about the passage of time and their children growing older and being independent, I say again that I cheer it.
You see, my job now is to prepare them for life without me. My goal is to show them how to accept the help of others but not be reliant on it. I choose to show them every day that there is determination and nobility in facing what life throws you. You may not be able to change the final outcome, but you can change what you do to be ready for it. The strongest way of teaching this right now is by living my life deliberately, making choices and showing them the best I can be. This doesn’t mean denial. Nor does it mean I don’t lose my temper or raise my voice or fall apart sometimes. To be emotionally numb or invariable in my response to what is happening is not healthy. I try to show them that expressing what they feel is a better option. Emotions of anger and sadness and grief and fear are fine to have. It’s beneficial to talk about them, but dwelling on them won’t make things better. Acknowledging their reality, their truth, their basis is what’s needed.
As I always say when I get bad medical test results: a short pity party is good. Then you have to pick yourself up and move on.
 It has been almost eleven months since my diagnosis of stage IV breast cancer, and there isn’t a day that goes by that is free from concern. I notice myself being more and more affected by the daily chemotherapy, feeling more fragile, more vulnerable. I have already had one bad respiratory illness this summer, and I worry about the school year and all of the potential colds and infections that will be transmitted. I don’t want to think about the ways cancer affects my daily life, but I must. The decisions I make about activities, treatments, and chemo all directly affect my life… both in length and quality.
It has been almost eleven months since my diagnosis of stage IV breast cancer, and there isn’t a day that goes by that is free from concern. I notice myself being more and more affected by the daily chemotherapy, feeling more fragile, more vulnerable. I have already had one bad respiratory illness this summer, and I worry about the school year and all of the potential colds and infections that will be transmitted. I don’t want to think about the ways cancer affects my daily life, but I must. The decisions I make about activities, treatments, and chemo all directly affect my life… both in length and quality.
I push myself to do the most I can. I try to do all of the little things that add up to a full day: school supply shopping, back to school haircuts, camp laundry, new shoes, sports registrations, and walking the dog. I also request meetings with school administrators, coaches, and anyone new in my children’s lives for this fall that need to know how my kids’ home life differs from the one they had a year ago.
I’m a planner. I take comfort in routine, the familiar, the predictable. Unfortunately, those are now removed from my life forever. Yes, I know life always tosses everyone curveballs. That’s what life is. But I experience it in a whole new way. I have no way of saying life will ever return to “normal” or even a “new normal.” There will not be a “better”… I am not “sick” in that I cannot recover.
I still feel the drive to help, to counsel, to educate. But am finding it more difficult. I hate saying no but know I will need to start saying this more. In-person interaction is very difficult for me. While no one would know it to look at me, social interaction is extremely draining these days. I try to minimize contact knowing that when I am in public I am under scrutiny. People want to know how I am. They want to be reassured. They look at me for clues as to how things are. There is no reassurance I can offer. This is a disease of progression to the end, a story that will not have a happy ending.
I want the story that I am living to be a good one, to the highest degree it can be. I want the story for my family and friends to be one full of love, memories, and devotion. These people are the center of my world.
I want the story to be different from what it has been, different from what it will be.
As a writer I am used to editing. Revising. Changing what I don’t like.
But I can’t edit this story.
I can’t start it all again.
And so I write through it.
The only way out is through.
But this one… well, this one is quite simply going to have a sad ending, as many stories do.
August 6th, 2013 §
 Hi all,
Hi all,
I may not be posting much this month. Now that all three of our children are home from camp the house is busy and we are readying for school. Public school here starts the last week of August so we have less than three weeks remaining of lazy summer days. I will make sure to post anything important news-wise.
My tumor markers have not climbed any higher in the last two weeks though they still remain slightly elevated from levels a few months ago. Both of my oncologists feel my current chemo regimen of Aromasin + Afinitor is still working. Nonetheless, we would like to see if we can drive the number down further and erase that gain. We are still getting a sense of how much variation is normal with this imprecise test.
Side effects on this Aromasin/Afinitor combo are cumulative in severity, so the longer I am on it, the worse they will become. Currently my major issues are fatigue, immunosuppression (making travel and being in public places risky), mouth and tongue sores, joint pain, muscle aches, skin breakdown, itchy scalp, sun sensitivity, high cholesterol, high triglycerides, increased blood pressure and rapid heart rate. Loss of appetite and associated weight loss are also factors. Yes, I know: to look at me you’d never know all of these plague me. I try not to talk about them too much but they are there.
Because I know many readers will be interested in potential remedies for some of these problems, I should say that I do have all of the treatments I need to deal with these side effects. Some of them are just the way it is, and you have to just adjust if possible. Others like mouth sores and skin/scalp issues can be very successfully treated with topical steroid ointments and liquids (some believe coating the Afinitor pills with food prevents mouth sores but this is actually just a coincidence. It’s not the contact with the mouth that causes the sores, it’s the mechanism of action that does. Blocking the mTOR pathway causes oral mucositis and stomatitis. Starting initially on a smaller dose and working up to the final one does seem to help with the initial outbreak of sores though). Walking helps both the joint pain (despite initial pain) and fatigue, while occasional Ativan helps the blood pressure, heart rate, loss of appetite, and some muscle issues. These are some of a few of the things that my oncologists and I have found to help.
One of my oncologists told me I was “at the precipice” with my side effects; my body could not tolerate a higher dose (currently I take 25 mg of Aromasin and I alternate 5 and 10 mg doses of Afinitor to average 7.5 mg/day). A meeting with my other oncologist today yielded a decision between that I would increase my chemo dose ever-so-slightly to see if I can tolerate it while hopefully get a response.
This type of situation is where the art of oncology comes in. I give a liberal interpretation to the term “art.” I think it’s educated guesswork, creative thinking. The science is the foundation but the application and choices are sometimes educated guesses.
We don’t know if a small increase will affect the tumor markers. It might. It might not. Can my body handle more? That’s an unknown too.
I think of it like the old fashioned scale in the doctor’s office– the one with the weighted bars that you slide left and right until they balance. The nurse gets close to the target, then nudges the bar bit by tiny bit until just the right balance is achieved. This is what we are trying to do: balance quality of life (side effects) with maximum efficacy. Where that line is, we do not know. It varies for each person.
We’ll test again in another week (two weeks since my last one), but it’s unlikely we would see any result that quickly. At least we will see if the markers are continuing to hold steady.
As far as this website, I have many ideas brewing for blogposts soon. Readers have also contributed some great ideas and asked questions that I will do my best to answer.
As always, thank you for the continued support.
July 29th, 2013 §
 A flash of red amidst the green summer grass:
A flash of red amidst the green summer grass:
a lone leaf, blazing in autumn clothing, a vivid premature announcement of a change of season.
Perfectly waxy, thick and juicy, it could not have been there long.
It is, I realize, the color of my mother’s lipstick. The color she has worn every day of my life. Perfectly fitting for the moment…
I turn 44 today.
I do not know how I feel about this fact.
The day I turned 43 was a lifetime ago, surely not just one year. I did not know I had metastatic breast cancer then. I was ignorant and blissful.
I had no idea what my life would be when I reached this birthday.
I have no way to know what it will be when I reach the next. I do believe I will see it though.
I am in limbo at the moment, waiting in the next few weeks to see if my current chemo has stopped working. I do not know if I will need to move on to something else to try to buy myself some time.
That is, you see, my only wish: more time. That is what I wish for today.
Time with my husband. Time with my children. Time with my parents and brother.
Time with my friends.
Chances for memories.
Opportunities for more.
I will keep trying to give a face and a voice to this disease.
There is poetry in the human experience.
I will keep trying to find it, document it, and also help others.
One way I have tried to help is by setting up a research fund at Memorial Sloan-Kettering.
If you can spare a few dollars and want to donate them to research on metastatic breast cancer, you can do so here. I don’t directly ask for donations often, but on this day I will.
I am glad to see 44. But there is inherent sadness in birthdays now.
Cake,
balloons,
the wish that comes true if you just close your eyes and blow out the candles…
if only it were so.
And so there is an anachronistic flash of red,
a moment of color.
I am that leaf,
released from the tree before its time,
floating downward,
coming to rest where it has no earthly business being,
nestled in the green summer grass.
July 19th, 2013 §
 They say that bad news is easier to deal with than uncertainty. I do believe it’s true. Give me something to deal with and eventually I figure out how to cope with it. I still am figuring out how to cope with a diagnosis of stage IV breast cancer. That one may take me the rest of my life. In that way, I hope it takes me a long time to figure it out.
They say that bad news is easier to deal with than uncertainty. I do believe it’s true. Give me something to deal with and eventually I figure out how to cope with it. I still am figuring out how to cope with a diagnosis of stage IV breast cancer. That one may take me the rest of my life. In that way, I hope it takes me a long time to figure it out.
The evil of “waiting” is a popular topic among those with illnesses. We spend an awful lot of time waiting. We have copious amounts of time in waiting rooms, exam rooms, lab offices, hospital admissions, chemo rooms and on and on. Then there’s the other kind of waiting: test results, scan results, waiting to see if treatment is working, time elapsed to see if abnormal test results are a fluke.
I’m in one of those waiting periods right now. My blood test this week showed an increase in tumor markers. This usually signifies that chemo is not working well anymore and the amount of cancer is increasing. However, as I’ve discussed many times before, this test is not precise. There is a reason it isn’t a screening tool to see if someone has breast cancer. It’s not a great test, but it’s one of the only ones we have. I’m not going to mention particular numbers here because the variation among individuals is so great and interpretation of trends over time is important and I don’t want anyone to be comparing their numbers to mine without a doctor’s help.
The jump in number was more than what can just be dismissed as normal fluctuation. But one blip does not a chemo failure make. A few months ago I had a few rises over the course of six weeks before my oncologists decided this was picking up resistance to chemo even before my scans showed any change. We try to keep ahead of it. My choice to monitor often and closely is not the right choice for everyone. Not all doctors would even agree to such a schedule. Each person finds the balance of time and testing that works for them.
So, for now I wait. We recheck, see what the data points are. One anomaly won’t be reason for an immediate change in treatment with my team. I’ve been through this once before, watching slow rises and then needing to change chemo. I didn’t think it would come again this soon. I’m hoping it hasn’t.
I hope for the best, I prepare for the worst. That’s all I can do.
But the waiting? The waiting is a nightmare. But I do always recognize that in that wait there is hope, because waiting is time.
If hoping and wishing could make things so I’d be cancer-free, or at least with chemo working for decades.
If wanting something could make it so…
Oh… there’s a long list for me on that one.
July 14th, 2013 §
 I never learned how to juggle. I never could master the coordination of having control of one thing while letting go of two.
I never learned how to juggle. I never could master the coordination of having control of one thing while letting go of two.
And yet, in my life, I am asked to do this daily. Three children, a husband, a house, the constant ebbs and flows of life and family and the demands those things take. Add stage IV breast cancer to this mix and it’s a daunting task at best.
“Too painful to think about” is something others can afford to say or think about those like me.
But I cannot. My body does not let me.
Perhaps having hair, looking healthy, betrays me.
Perhaps people forget what my body is enduring.
Perhaps they forget on a daily basis the struggle it is for me to do what I need to do. On some days the hardest task I have is the mental component of trying to deal with this all.
They do not know that while I drink my coffee in the morning and type an email I am prone to worry. I wonder if pain in my side or my back or my neck is cause for concern. I am mentally comparing the location of the pain to the bright flashes on the latest PET scan. I try to remember my body’s details on that scan. I create a split screen in my mind. I contemplate if the spots align, if they don’t. I have memorized the words in the radiology report. When I want to torture myself I recite them.
There is no “moving past cancer” anymore or counting down to the end of chemotherapy. There will be no day of claiming victory and yet my victory is defined by each day. Winning is not possible, its re-definition now just seeing how long I can keep running, outsmarting the cancer that’s here to stay.
I waved a triumphant flag six years ago. I was done with surgery, treatment. My chances of a recurrence or worse, a metastasis: small, small, small. Single digit. The odds were in my favor. “Look where those odds got me!” I scream inside.
I serve as a terrible, disturbing reminder to those just starting treatment: you can’t be sure. You can’t get cocky. You can’t ever be positive that you are done. Perhaps you live your daily life that way, but it can happen. Even years later, it can happen.
That wily son of a bitch can lay in wait, cells silent, dormant for a while. And then, when you least expect it, spring forth to attack, to ravage, to ruin all you know is true. This is why I bristle when people with my particular kind of cancer say they are “cured.”
I hesitate when people ask me how I am.
I know they want to believe I am okay.
Even for today.
They want to believe there will be a happy end to the story.
But there cannot be.
This is not my middle age. I will not be that lucky. While others complain of gray hair or wrinkles or saggy bellies I long for them. I want to earn those badges.
I want to flaunt my age.
But let me flaunt a number that begins with a 5… or 6… or more…
I now know this is why my doctor had that look on his face when he told me the news last October that my cancer had metastasized. This is why, when he gave me the news, he let me cry and swear again and again and again when every word in the English language but “Fuck” left my vocabulary.
This is why a particular doctor I know looks at me with sadness in his eyes when I see him, when he hugs me, when he tells me “you look good.”
That doctor looks at me like that because he has the curse of knowledge: he knows how this will go.
He knows. He knows this story, he sees it daily. He knows what’s coming. He doesn’t want me to see the ending but it will come. All we are doing is pushing the “pause” button as many times as we can. When I hug him I feel it. The regret. The pain. He knows what waits for me. It makes me sad to see him in the hall sometimes, as if that feeling can be transferred between us in a look, a hug, a touch. But that compassion, that pain… well, those are honest moments.
Perhaps I ramble today. Perhaps my weary body and mind make no sense. Perhaps I should hit “delete” and send this down the drain. But this is all part of my story. If I am feeling it, I know somewhere someone else can relate to it too.
Every day is a struggle of one kind or another. I am doing the best that I can.
And oh, how I wish I could forget. How I wish I could forget.
July 5th, 2013 §
 Something happened to my brain when I heard the words “Your breast cancer has metastasized.” Suddenly, irreparably, it became a sieve. Surgical menopause without the option of hormone replacement seven years ago started the process. But mental anguish and immediate, lifelong chemotherapy been major contributors to my Swiss cheese mind.
Something happened to my brain when I heard the words “Your breast cancer has metastasized.” Suddenly, irreparably, it became a sieve. Surgical menopause without the option of hormone replacement seven years ago started the process. But mental anguish and immediate, lifelong chemotherapy been major contributors to my Swiss cheese mind.
I used to read a lot. People think of me as a reader. I am sorry to say I’ve become a fraud.
I love to support authors and their books. That has not changed. It never will.
But when it comes to what I’m actually reading (and finishing)… well, I have a confession to make: it’s not much in the past nine months.
My mind jumps all over the place. It simultaneously wants quiet but is restless. It craves nothingness and distraction. It is hard for me to sustain long conversations; I find them exhausting now. This is one reason Twitter has remained such a wonderful social medium for me; it is defined by short chats that can be stopped and started at will.
When it comes to reading, however, I am having trouble. I hope this ability will return. I spend my focused time writing when I can. Even then, as readers here know, I almost always write brief pieces, expressing thoughts in as few words as possible.
When I was first diagnosed with breast cancer and underwent chemo in 2007 I didn’t read either. I hear from so many people that this is how they felt, too. Those who are newly-diagnosed think they will spend their time catching up on books they want to read during chemotherapy or after surgery. It just rarely happens: either your brain is in a fog or you feel rotten. When you feel good, you want to get out and do things with your family and/or friends.
My current stack of “am reading” and “to be read” is shown in the photo above: books by Dani Shapiro (am reading), Kate Atkinson, Rosie Schaap, and Meg Wolitzer (to be read). I’ve cleared out shelves and shelves of books that I know I won’t get to and given these treasures away. It really made me sad to see so many books there, mocking my isolation: tangible reminders of things I will leave undone. And yet, I saved a bookcase or two of books I still want to read. I won’t give up hope completely.
So now I turn it to you, readers: Do you go through phases of reading? What have you noticed about your reading habits when you had bad news? Health issues? Medical treatment of some kind?
On the flip side, what happened to your reading habits after happy events? I didn’t read after the birth of each of my children: middle of the night feedings were accompanied by nodding off, not turning pages of a book. I’m not an audio book person, I should specify. I know how wonderful this format can be, it just doesn’t work for me. I either fall asleep (chemo fatigue and the sound of someone reading to me… isn’t that how we prime our children for bedtime, after all?) or my mind does its trademark wandering and I have to keep rewinding the story.
The beautiful thing about a book is that it endures. It will wait for you. Like a good friend, when you are finally ready, it will share itself with you.
July 1st, 2013 §
 Like dollhouse rooms left abandoned,
Like dollhouse rooms left abandoned,
The rooms stay tidy:
Beds made tight,
Pillows square,
Hampers empty.
It’s been one week since the children left for camp.
Littlest Tristan was due back yesterday but a few days ago he said he was having so much fun he wanted to stay another week.
I realized this week that after being sick for the previous two that I needed this time to catch up, to rest, to regroup.
I miss them but am so glad they are having fun doing what they love.
I pack up care packages,
write letters,
wake in the middle of the night and mentally picture our children sleeping in cabin beds.
Our dog Lucy follows me, sleeps in my room now, not Paige’s.
She doesn’t want to be alone and stays within feet of me every moment.
I tell her it’s okay:
The kids will come back.
The rooms will get messy again.
There will be crumbs dropped at the dinner table and car rides galore.
Paige and Colin and Tristan will come back tired and dirty and happy.
They will come back.
They will.
That is the key.
I think of absence like a hole:
How different it is when it’s temporary and filled with happiness,
Rather than when that hole is a pit of grief. Of ache. Of loss.
The way it will someday be for them.
June 26th, 2013 §
 I’ve again invited my mother, Dr. Rita Bonchek, to write a piece for the blog. Her previous posts on the difference between guilt and regret, grieving the death of a parent, what it’s like to read my blogposts about cancer, and how to help children understand death have been well-received. As a psychologist specializing in grief and loss I think her perspective and ability to share insights are welcome additions to the posts I make. I know that she gains comfort from talking with other parents who have children with cancer and sharing their feelings about the way that cancer has affected their roles as parents (and often as grandparents). Her post appears below.
I’ve again invited my mother, Dr. Rita Bonchek, to write a piece for the blog. Her previous posts on the difference between guilt and regret, grieving the death of a parent, what it’s like to read my blogposts about cancer, and how to help children understand death have been well-received. As a psychologist specializing in grief and loss I think her perspective and ability to share insights are welcome additions to the posts I make. I know that she gains comfort from talking with other parents who have children with cancer and sharing their feelings about the way that cancer has affected their roles as parents (and often as grandparents). Her post appears below.
I think the only thing I would say that I might disagree with here is that I don’t think it has to always be a one way street. Mom refers to a time when I was helping her with problems she had in her own life. Yes, perhaps it’s important to be aware of when you are asking your child for help or advice. However, if this is the way your relationship is (ours is, for example), then I believe that maintaining some of this dynamic adds to the sense of “normalcy” that may be elusive but also can be comforting to both parties. That is, if I am not in an immediate medical crisis, helping my mother with a problem she is having feels good to me, rewarding, reminiscent of the way things were before. If the street is always one way, that adds to the feelings of separateness between us, a strong reminder that everything is different.
A suggestion we both have is to focus more on parents taking care of themselves, finding ways to cope in a way that is right for them. Certainly parents and children do not always have the same strategies to deal with medical crises. The parent also may need support to deal with his/her grief during this fragile time. Individuals may find help in talking to a therapist or other supportive figure or attending a support group for parents.
There are constant ebbs and flows in the parent/child relationship based on how treatments are going, anxiety about upcoming tests or bloodwork, and the side effects of treatments. It may not always be clear how much the parent needs to be parent at any given time. Open communication is so important. One of the hardest conversations my mother and I had recently was one in which I openly laid out some ways in which she could be more helpful to me now. That conversation led to a wonderful new phase of support. She feels good that she knows better what I need, how to be helpful to me and to my family. I cannot expect her to be a mind-reader, and the ways that I need support change with how my treatments are going. I will be undergoing treatment for the rest of my life, so it’s important that we are as honest and supportive of each other as possible. I know that she has her own challenges in dealing with my diagnosis. She feels good now knowing some of the things she can do that are most helpful. I truly believe that is what makes a parent feel good is to know they are a help, rather than an additional source of stress for their child during this difficult time.
My mother and I both hope that this piece will be an introduction to this topic. There is so much to say about changing relationships during medical crises. Perhaps today’s post will allow you to raise some of these topics with a family member.
……………………………………
Dr. Rita Bonchek writes:
Throughout this blogpost, I repeatedly refer to children. Even though adult in years, they are our children. When they are diagnosed with cancer, the relationship between parent and child will, by necessity, change. I would like to suggest how parents can strengthen the relationship and cope more effectively at this time.
When Lisa completed cancer treatment after her initial diagnosis (double mastectomy and chemotherapy in 2007, oophorectomy in 2008), everyone, including her doctors, believed that there was an infinitesimal chance that the cancer would return: that period of time was in the past and life would move forward. When the cancer returned in the form of an incurable metastasis in 2012, we were all devastated.
Families have one type of relationship when all of its members are healthy and a different type when one member is ill. But cancer isn’t necessarily just being ill for a period of time, recovering and continuing on with life. Cancer can be a life and death everyday concern. So, what happens? The conversations change because references to cancer are screened , levity is uncomfortable because how can one laugh about trivial jokes when something so serious is occurring and discussions that involve long-range planning are avoided since how long will long-range be.
Who we were as parent and child before the diagnosis of cancer is not who we are and become after the devastating news. The prior carefree mutual relationship now shifts from both of the parties interacting and sharing problems and concerns to only focusing all attention and sensitivity towards the child. There is now a one-way street. How could this not be? When one asks the question “Whose needs are being met?” it must only be the one who lives with the cancer. The goal is, as much as possible, to reduce stress and tension between mother and child but, most importantly, within the child.
There are some tensions that occur when a parent offers to help a child with household chores, fixing meals, carrying packages, etc. A child’s snappish response of “I can do it myself” may indicate that to accept the offer is to admit a weakened condition. Or, any offer to help may cause reminders that at some time sooner or later that help will be needed. It may be better just to do the chore without asking as in folding laundry, unloading the dishwasher, making a meal that could be frozen if the gesture is not accepted. It is MOST important that we do not take personally such behaviors as negativity or curtness. There can be mis-directed anger at a parent instead of directed, expressed anger at the overwhelming madness-sadness of the cancer diagnosis.
It can be helpful to establish ground rules. The parent can ask “What CAN I do for you that would be helpful?” “What should I NOT do that might be upsetting to you?” Those of you who read this blog-post will surely have suggestions that all of us, who are trying to function each day as best as possible for ourselves and for our children, can benefit from reading.
From the day of the diagnosis, our worlds have changed irrevocably for the worse and we must adjust. I may sound as if I knew exactly what to do and employed suggestions proffered. Not so. Just ask Lisa. I let her down. I had personal problems during the time after her diagnosis of metastatic breast cancer and I vented and asked for her advice as she was trying so hard to just get by.
I felt only Lisa knew the participants well enough to understand my dilemmas and to help me. Time after time, I apologized, I vowed that I would not involve her again and she forgave me. But once was not enough, even twice was not enough, for me to learn my lesson and to seek help elsewhere. If I had remembered to ask myself “Whose needs were being met?,” I hope I wouldn’t have placed Lisa in that position. Our children may no longer be as available to support us.
When I was in practice as a psychologist who specialized in grief and loss counseling, I tried to help my patients to understand, process and deal with major losses. I often explained to them that denial was an effective coping mechanism if it allowed them to absorb the overwhelming loss little by little, bit by bit. But denial cannot be total and the reality of the situation must at some time be acknowledged. So, although I do recognize the possibilities of breakthroughs in medical science, I do not believe in nor count on miracles.
I will let my thoughts go a certain distance into the future when I must, but I function day by day as a way of living . I choose not to focus on what may occur in the future because it may not occur. What a waste of time and energy that would be. I cannot focus on the possible downturns during the treatment, on any pain or suffering Lisa could be experiencing but is not telling me about.
The reality is that though I can support and comfort her, there is nothing I can do to make her physical and emotional suffering go away. If I indulged in this negativity and worry about Lisa in my everyday life, I would have no life. I try to remember- not always successfully- that worrying benefits no one. If my worrying could provide even a tiny extension of Lisa’s life, I would worry myself sick.
A line in Joyce’s “ Ulysses” states this emphasis on the present: “Hold to the now, the here, through which all future plunges to the past.”
To derive satisfaction from life, Lisa and I agreed that auditing classes at Franklin & Marshall College would distract me with an activity that would challenge me and bring me satisfaction. And so it has. The last thing we want our children to do is to worry about us. Whatever we do for ourselves, we do for them. Find some interest or activity that gets you through each day.
Lisa and I have quite different personalities and behaviors. As her readers know, she is very open in describing her thoughts and feelings. In contrast, I was a very private person. When Lisa first started writing, I was uncomfortable seeing private information about our family being disclosed publicly and shared with people I did and did not know. But, very soon, I began to appreciate the role that Lisa’s writing played and continues to play in her life and the lives of her readers. And so I changed and re-evaluated my stance on privacy. In answer to the question “whose needs were being met?” I substituted my privacy desire for Lisa’s openness. I stand with Lisa to help cancer patients and their loved ones live with cancer and not die from cancer.
Our daughter, Lisa, is an incredible daughter, wife, mother and friend. I cannot and will not imagine living my life without her.
June 24th, 2013 §
 Today is the eight year anniversary of the death of Suzy Rosin. Suzy was special to many different people as anyone who has read the book If You Knew Suzy: A mother, a daughter, a reporter’s notebook knows. One of the ways she is most special to me is that she is the mother of my friend Katie.
Today is the eight year anniversary of the death of Suzy Rosin. Suzy was special to many different people as anyone who has read the book If You Knew Suzy: A mother, a daughter, a reporter’s notebook knows. One of the ways she is most special to me is that she is the mother of my friend Katie.
I first wrote about these two extraordinary women back in June of 2010 after reading Katie’s memoir about coming to know her mother’s diverse legacies after Suzy died from lung cancer at age 60.
Revisiting old blogposts takes me on an emotional rollercoaster. Being on the other side — having incurable stage IV cancer — gives the pieces a whole new meaning.
This post captures my fervent wish to document my thoughts and feelings for my children. I still feel a strong desire to be understood. I think in many cases people with cancer do not feel understood. Katie’s dedication for the book echoes this wish: “To my mother’s grandchildren, so they may know her.”
Katie and I have become friends. Great friends. We talk about Suzy. We talk about french fries and silly socks and Pilates. We talk about her work and we talk about our kids. We talk about cancer. We talk about the most frivolous parts of life and the most serious. As I write below, “Even after her death, Suzy has the lovely ability to inspire, to entertain, to be present.” In life, so does her daughter, Katie.
………………………………….
Originally published June, 2010
There comes a point in your life when you realize that your parents are people too. Not just chaffeurs, laundresses, baseball-catchers, etc.– but people. And when that happens, it is a lightbulb moment, a moment in which a parent’s humanity, flaws, and individuality come into focus.
If you are lucky, like I am, you get a window into that world via an adult relationship with your parents. In this domain you start to learn more about them; you see them through the eyes of their friends, their employer, their spouse, and their other children.
Yesterday I sat transfixed reading Katherine Rosman’s book If You Knew Suzy: A Mother, A Daughter, A Reporter’s Notebook cover to cover. The book arrived at noon and at 11:00 last night I shut the back cover and went to sleep. But by the middle of the night I was up again, thinking about it.
I had read an excerpt of the book in a magazine and had already been following Katie on Twitter. I knew this was going to be a powerful book for me, and I was right. Katie is a columnist for The Wall Street Journal and went on a mission to learn about her mother after her mother died in June, 2005 from lung cancer. In an attempt to assemble a completed puzzle of who her mother was, Katie travels around the country to talk with those who knew her mother: a golf caddy, some of her Pilates students, her doctors, and even people who interacted with Suzy via Ebay when she started buying up decorative glass after her diagnosis.
Katie learns a lot about her mother; she is able to round out the picture of who her mother was as a friend, a wife, a mother, a strong and humorous woman with an intense, fighting spirit. These revelations sit amidst the narrative of Katie’s experience watching her mother going through treatment in both Arizona and New York, ultimately dying at home one night while Katie and some family members are asleep in another room.
I teared up many times during my afternoon getting to know not only Suzy, but also Katie and her sister Lizzie. There were so many parts of the book that affected me. The main themes that really had the mental gears going were those of fear, regret, control, and wonder.
I fear that what happened to Suzy will happen to me:
My cancer will return.
I will have to leave the ones I love.
I will go “unknown.”
My children and my spouse will have to care for me.
My needs will impinge on their worlds.
The day-to-day caretaking will overshadow my life, and who I was.
I will die before I have done all that I want to do, see all that I want to see.
As I read the book I realized the tribute Katie has created to her mother. As a mother of three children myself, I am so sad that Suzy did not live to see this accomplishment (of course, it was Suzy’s death that spurred the project, so it is an inherent Catch-22). Suzy loved to brag about Katie’s accomplishments; I can only imagine if she could have walked around her daily life bragging that her daughter had written a book about her… and a loving one at that.
Rosman has not been without critics as she went on this fact-finding mission in true reporter-style. One dinner party guest she talked with said, ” … you really have no way of knowing what, if anything, any of your discoveries signify.” True: I wondered as others have, where Suzy’s dearest friends were… but where is the mystery in that? To me, Rosman’s book is “significant” (in the words of the guest) because it shows how it is often those with whom we are only tangentially connected, those with whom we may have a unidimensional relationship (a golf caddy, an Ebay seller, a Pilates student) may be the ones we confide in the most. For example, while Katie was researching, she found that her mother had talked with relative strangers about her fear of dying, but rarely (if ever) had extended conversations about the topic with her own children.
It’s precisely the fact that some people find it easier to tell the stranger next to them on the airplane things that they conceal from their own family that makes Katie’s story so accessible. What do her discoveries signify? For me it was less about the details Katie learned about her mother. For me, the story of her mother’s death, the process of dying, the resilient spirit that refuses to give in, the ways in which our health care system and doctors think about and react to patients’ physical and emotional needs– all of these are significant. The things left unsaid as a woman dies of cancer, the people she leaves behind who mourn her loss, the way one person can affect the lives of others in a unique way… these are things that are “significant.”
I woke up in the middle of the night thinking about the book. My head spun with all of the emotions it raised in me. I think that part of the reason writing has become so important to me is precisely because I do realize that cancer can return at any moment. And if you don’t have an author in the family who might undertake an enormous project as Katie did, where will that explanation of who you were — what you thought — come from?
Is my writing an extension of my desire to control things when cancer has taken away so much of this ability?
Is part of the reason I write an attempt to document my thoughts, my perspective for after I am gone… am I, in a smaller way, trying to do for myself what Katie did for her mother?
If I don’t do it, who will do it for me?
And in my odd way of thinking, am I trying to save anyone the considerable effort of having to work to figure out who I was– deep down?
My blog originally had the title “You’d Never Know”: I am telling you things about myself, my worldview, and my life, that you would otherwise have no knowledge of. One of the things people say to me all the time is, “You’d never know to look at you that you have cancer.” After hearing this comment repeatedly I realized that much of our lives are like that:
If we don’t tell someone — share our feelings and experiences — are our lives the proverbial trees falling (unheard) in the forest?
What if you die without being truly understood?
Would that be a life wasted?
If you don’t say things for yourself can you count on others to express them for you?
Further, can anyone really know anyone else in her entirety?
After a loved one dies, there always seems to be at least one mystery person: an individual contacts the family by email, phone, or in person to say, “I knew your loved one: this is how I knew her, this is what I remember about her, and this is what she meant to me.” There are stories to be told, memories to be shared. The living gain knowledge about their loved one. Most often, I think families find these insights comforting and informative.
Katie did the work: she’s made a tribute to her mother that will endure not only in its documentation of the person her mother was (and she was quite a character!) but also in sharing her with all of us.
Even after her death, Suzy has the lovely ability to inspire, to entertain, to be present.
I could talk more about the book, Katie’s wonderful writing, and cancer, but I would rather you read it for yourself. I’m still processing it all, making sense of this disease and how it affects families, and being sad that Katie’s children didn’t get to know their grandmother. Katie did have the joy of telling her mother she was pregnant with her first child, but Suzy did not live long enough to see her grandson born. In a heartwarming gesture, Katie names her son Ariel, derived from Suzy’s Hebrew name Ariella Chaya.
I thank Katie for sharing her mother with me, with us. As a writer I learned a lot from reading this book. I’ve said many times recently that “we don’t need another memoir.” I was so wrong. That’s like saying, “I don’t need to meet anyone new. I don’t need another friend.” Truth is, there are many special people. Katie and Suzy are two of them.
June 22nd, 2013 §
 In these last remaining hours
In these last remaining hours
Before my children disappear
One,
Two,
Three…
In these last remaining hours before they go and spread their wings again,
Leave this nest,
I miss them already.
I put the dinner pots and pans away.
Wipe the crumbs from the table,
Load the dishwasher,
Play fetch with the dog.
I sit in the garden,
Listen to the wind in the trees,
The birds settling down before nightfall,
As we settle, too.
I tuck them in one last time,
Hear their doors click shut.
One,
Two,
Three.
Tomorrow night there will be no mess to clean,
No yelling upstairs that the TV has been left on again,
No trunks piled high with carefully labeled belongings in the dining room.
I will cry, I know.
Not because I am sad that they are going– no, that gives me great joy.
Children being children.
Forgetting stress at home and doing new and varied things.
I cheer their independence.
I will cry because I know they will always need me somehow and I just wish I could be there for them to outgrow
by choice,
by time,
by age.
I hear the mother bird in the tree calling out.
I don’t know to whom.
I will be like that tomorrow,
calling out,
with no child to hear.
June 10th, 2013 §
 I have my list of things I worry about.
I have my list of things I worry about.
First on my mind in the morning,
Last in my head at night.
And if I pop awake In the middle of the night?
Yes, the list is there too.
Across the aisle from me on the train to New York City last time sat a woman.
At one point on the journey she flipped huge black bug-eye sunglasses from the top of her head down over her eyes, her look now an insect dressed in designer clothes.
She reached in her purse,
grabbed a strand of worry beads and started kneading them.
With a rapid-fire reflexiveness she started moving one bead at a time .
Each only moved about half an inch down the string.
From the worry side to the safe side.
I could hear the rhythmic mantra of the beads again and again and again,
Quieter but still audible over the clickity clack pattern of the train itself.
I wondered what her worries were.
I wondered if she would add mine to hers.
Or trade with me, even.
Sometimes we need to do something with that energy.
For her it was tiny movements, thumb and forefinger
Pinching and sliding ivory beads on a round string.
We have our rituals when things get bleak. Some pray.
I do not.
There is a coping that comes with grief, a way to release the tension that grips us when things are bad.
Some days it does feel like it eats from the inside out.
When you must come to terms with what you fear
and what you dread
and all you want to do is lay down on the floor like a petulant two year old
and kick and scream about the unfairness of it all…
As if the universe gives a damn that life hasn’t been fair to you.
Clearly it doesn’t.
So I do not appeal to the universe to change what is.
I turn to my balms. I turn to research.
I turn to science.
I turn to determination and hope which are the last things I can cling to,
fingertip by fingertip,
like the cat on that iconic poster that says “Hang on, baby.”
Inner strength is sheer will.
My claws are firmly entrenched.
There is no other way to be.
There is no justice.
It’s up to me to come to terms with the weighted side.
That is where I live right now.
And so every day, when I wake up in the pre-dawn hours and contemplate my worry list and
come to terms with the day that is about to dawn,
I gather strength,
summoning it from its slumber.
“Here we go,” I say.
“Let’s do this.”
Another day is here.
I will see another.
Hang on, baby.
June 8th, 2013 §
 Two weeks ago we had a family photo session with my friend Julia Arstorp. Julia has taken numerous series of photos of us through the years and I really wanted to have updated photos of all of us. The children have changed so much in the past two years! I will share some of them throughout the next few months. I have updated my Welcome page of the blog with a few of them too. I know some of you only read these posts by email so you can always take a peek at the home page to see what’s new.
Two weeks ago we had a family photo session with my friend Julia Arstorp. Julia has taken numerous series of photos of us through the years and I really wanted to have updated photos of all of us. The children have changed so much in the past two years! I will share some of them throughout the next few months. I have updated my Welcome page of the blog with a few of them too. I know some of you only read these posts by email so you can always take a peek at the home page to see what’s new.
One of the photos I love most is this black and white one with our new dog Lucy, a Pembroke Welsh Corgi that we got in January. If you follow me on Twitter you know how much I love her. She is my first dog ever… the kids always wanted a dog but I wasn’t sure about the commitment. Clarke had a great Corgi named Pearl when we met so I knew the breed and loved their personalities. Lucy is two now and she has brought such joy to our lives.
 Most people who know me are shocked I not only let Lucy on the bed and throughout the house. My attitude is she is a part of our family so she gets to share. She’s not a big snuggler (prefers to lay next to you or under the bed) but we have had some great naps together over the past few months. She is great at fetch which is a lot of fun to watch as her little legs run so fast and her big ears get pinned back to her head as she scurries… she is fast on those little legs!
Most people who know me are shocked I not only let Lucy on the bed and throughout the house. My attitude is she is a part of our family so she gets to share. She’s not a big snuggler (prefers to lay next to you or under the bed) but we have had some great naps together over the past few months. She is great at fetch which is a lot of fun to watch as her little legs run so fast and her big ears get pinned back to her head as she scurries… she is fast on those little legs!
The end of the year is very busy now with school ending for all of the kids. Colin will graduate from elementary school and start at the middle school in 6th grade in the fall. Tristan will be going into second grade and Paige will be a high school sophomore (eek!). Right now we have baseball playoffs, karate belt testing, and some upcoming visits from family.
I’ve been managing the side effects from the new Aromasin/Afinitor regimen pretty well. Right now I’m still on 7.5 mg of Afinitor a day, my biggest problems from the drug combo are severe muscle and joint pain, thyroiditis (I also have Hashimoto’s Disease), loss of appetite with weight loss, and migraines. The mouth sores and head irritation have improved.
Bloodwork yesterday showed a drop in my tumor markers, an indication that it is still working now after about 2 months. This gives me a two week reprieve in worry. I really do live in two week increments right now. I’ve been able to do all of the things I need to do and most of the things I want to do. I am learning more and more the difference between these two things.
 I’ve attended every single one of Colin’s baseball games. I got all three of them to the dentist for checkups and their regular doctors’ appointments. I keep a regular schedule right now but try to rest more on weekends when I can. I am glad for the normalcy that my days mean to them and to me. We all know it’s not truly normal, of course, but the comfort of routine is real, especially to them. I find it hard to believe the last 8 months have been since my diagnosis of metastatic breast cancer.
I’ve attended every single one of Colin’s baseball games. I got all three of them to the dentist for checkups and their regular doctors’ appointments. I keep a regular schedule right now but try to rest more on weekends when I can. I am glad for the normalcy that my days mean to them and to me. We all know it’s not truly normal, of course, but the comfort of routine is real, especially to them. I find it hard to believe the last 8 months have been since my diagnosis of metastatic breast cancer.
I gave an interview to the Daily Beast this week about Komen’s cancellation of many of their walks this year because of drops in funding despite Nancy Brinker giving herself a pay raise to $685,000 a year. I wish the piece had gone into more depth about the lack of funding for metastatic research, but I still think some good points were used from the interview. You can read it here.
If you are looking for a place to donate money for breast cancer research, I do have a donation page at Sloan-Kettering which funnels money to metastatic breast cancer research. You can see the page here. It has raised about $17,000 since last fall.
I hope you all have a good weekend.
Find a bit of joy in the world. Share it. If you can’t find it, create it…
June 4th, 2013 §
 I just want to see my son play baseball,
I just want to see my son play baseball,
Watch him wave at me when he’s on base.
I just want to take my daughter shopping for makeup,
Applying powder to her porcelain skin.
I just want to read with my youngest one,
Snuggled up in bed together turning pages of a book.
I just want to grow old with my husband,
Continue to share our lives as we have for twenty-two years already now.
I just want to sit in the garden when we are old.
I just want to talk about the good old days.
I don’t want to read about mTOR inhibitors or side effects or months of disease-free progression.
I want to read beach fluff and skim through cheesy magazines.
I want to get a pedicure and have a nap in the chair.
I want choosing the color of my nail polish to be the toughest decision I have to make for a day.
I don’t want to read reports from the ASCO conference or tweets about new research findings.
I just want it to go away.
But it can’t.
It won’t.
I will never know another day of my life without metastatic cancer or chemo or treatment or dread.
But I will search for joy.
I will.
I will do what I can every day to find that joy,
And if I can’t find it I will make it.
This is my pledge,
This is my promise.
For them.
Some days it is hard to do.
Some days fear and sadness are too much.
Some days I do not know how I will do this with grace,
But I will try.
I must make the most of this time:
Helping others, educating, writing.
I know no other way to do this.
But it’s the hardest thing to do.
I cry, I give in to the emotions, but only for a few minutes.
No good can come from that.
I gather strength.
I re-commit.
I go on living.
The bad days will come someday.
But that day is not today.
That time is not now.
And so I am a parent, a wife, a friend, a sister, a daughter, a writer, and everything else I have been until now.
That is who I am.
That is who I will continue to be.
For as long as I possibly can.
May 31st, 2013 §
 This afternoon I will attend my youngest child’s Field Day. It will be a steamy 93 degrees here and I will join parents as we stand around and chat while we clap for our children and hug their sweaty bodies and remind them to drink lots of water.
This afternoon I will attend my youngest child’s Field Day. It will be a steamy 93 degrees here and I will join parents as we stand around and chat while we clap for our children and hug their sweaty bodies and remind them to drink lots of water.
It is always in these group events that so many of us feel like outsiders. It is often when surrounded by many people we are most aware of being alone. For me, this has never been more true than during the past 8 months since my diagnosis with stage IV breast cancer.
I return again and again to the desire to escape, the need to flee, the pull toward being somewhere else. The refrain in the new song I am co-writing with Doug Allen is about this need we all have, regardless of the cause, to take moments during the day where we just “check out” for a bit. It says:
I take a trip inside my head,
I don’t know where I go.
Somewhere else,
Anywhere else,
Far from things I know.
There are days when I want to be the ostrich, when I just am so overwhelmed with things that I can’t be on social media, returning emails, or even talking. I just am still. I notice that I rarely read anymore, even television can’t capture my attention. I sit in silence a lot, and when I have the opportunity I write or work on the songs.
I take those trips inside my head.
The pull of educating and informing is too strong to allow me to stay hidden away, though. Social gravity pulls me back. Sharing and documenting fuel me. I take my anger, my sadness, and my grief and I send them out into the world in constructive words and deeds. I can feel powerless and without control in many ways about what is happening to me but I always feel that I can control my reaction to these things. This is my lesson to the people in my life.
There is a scene in the film Children of a Lesser God where William Hurt’s character jumps into a pool to try to experience utter silence the way that his deaf girlfriend does. He wants to know what that feels like. He quickly realizes, however, that this won’t work. He knows when he rises to the surface he will once again hear sound. He can’t live what she lives. He can’t share her loss in that way.
Antoine de Saint-Exupery wrote, “It is such a secret place, the land of tears.” Most mornings I stand in the shower for a while longer than I need to. I listen to the water, I think about the day, I am grateful to have another. I know I will have more days. For those few minutes I take a trip inside my head. I gather my strength, I focus on the work to be done.
I turn off the water, I step out of the enclosure, and I rejoin the world of the living. That’s what I am doing every day: living with metastatic cancer.
May 27th, 2013 §
Today is Memorial Day. Each year my letter to troops stationed overseas is similar. Each year I question whether I should write something new, if it’s “cheating” to say the same thing. In the end I realize that thank you never gets old, it never needs to be re-written. Thank you doesn’t have an expiration date.
This year we went to buy items for the care package drive sponsored by the Darien Little League. Volunteers collect supplies including toiletries, non-perishable food, and games and send them to soldiers far from home.
My letters always have the same theme: bravery– chance or choice? I don’t know if the soldiers find my musing on this distinction weird in a letter, but they must ponder the topic of bravery as often as I do.
………………………………………
May 27, 2013
Dear Servicemen/women,
My family and I are sending you some supplies on this Memorial Day Weekend. We want you to know that we have not forgotten you or the sacrifice you are making every day to be away from your own families and in harm’s way. It’s not much, but perhaps knowing you are in our hearts and minds will help.
Six years ago I was diagnosed with breast cancer. I was in remission for more than five years and now my cancer has metastasized to my bones and lymph nodes. It’s not curable. As I go through treatment, people called me brave. I don’t think I deserve it. “Brave” is not a word you used about someone like me. I have gotten cancer by chance and I am dealing with it, the best I can.
But soldiers? You are brave. You have a choice—you put your lives on the line after making a conscious decision to do so. You know the danger and you do it anyway. To me, that is true bravery, true heroism.
Seeing danger and making the choice to proceed anyway is precisely how I define bravery. We all find ways to deal with the fear of death. We know the uncertainty that lies ahead. We see the bravery in others before we will see it in ourselves.
What underlies bravery: chance or choice? Can both?
Are we just hesitant to see the quality in ourselves? Are we just modest? Do we just act the way we need to, to get the job done?
I think when you choose to throw your hat in the ring, that choice counts for something.
That makes you brave.
That’s what makes soldiers heroes.
Happy Memorial Day to you. And thank you for your continued service to our country.
Lisa Bonchek Adams
May 24th, 2013 §
 It’s Friday! I want to put a post up today because I know it’s been a while and people worry when I am not making posts. All is fine, it’s been a very busy week with a lot of routine medical appointments. Side effects from the new chemo are starting in and phrases like “mouth sores”, “high cholesterol,” and “follicular head pustules” make me certain that the person who called it “crazy, sexy cancer” was delusional about what cancer really is. There’s a lot that’s crazy but I don’t personally find a lot of sexy in it.
It’s Friday! I want to put a post up today because I know it’s been a while and people worry when I am not making posts. All is fine, it’s been a very busy week with a lot of routine medical appointments. Side effects from the new chemo are starting in and phrases like “mouth sores”, “high cholesterol,” and “follicular head pustules” make me certain that the person who called it “crazy, sexy cancer” was delusional about what cancer really is. There’s a lot that’s crazy but I don’t personally find a lot of sexy in it.
I’m getting help from my team in dealing with all of the side effects and have more appointments with more specialists in the next few weeks. For now things are stable and the next two weeks will proceed as planned. I’m still on Aromasin (25 mg/day) and Afinitor (7.5 mg/day). It’s the Afinitor that’s kicking in with my various problems. My tumor markers have shown a response to this combo over the last 6 weeks so we continue with it for now. I also received my monthly injection of Xgeva to strengthen my bones.
I wish you all a good Memorial Day weekend, especially our military personnel and their families.
The photo above is from 2002 by the way… where have eleven years gone?
I also want to mention that my last post, “There’s No Room for That in This (Six Minutes)” is the foundation for what is now a song titled “Six Minutes.” Over the past few weeks musician Doug Allen and I have been working hard on it and we’re almost done. I wrote the lyrics and he found the perfect music to bring those words to life. We are both so proud of the song and will be sharing in the future. His latest CD is available now and I just love it; it has two songs that have been on movie soundtracks… who knows where “Six Minutes” might land! More to come on this project.
………………………………
I get a lot of emails and comments with questions about cancer and how to help those who have it. Let me say clearly that I never think I speak for everyone with cancer. I do believe that asking questions is good, and even if you don’t think my answer is right for you, at least you might look at the issue a different way and clarify your own thoughts.
If people like this format I may continue to post letters/responses more often. I have often thought we need a grief/loss/illness etiquette column and I’ll gladly do my best to help.
This week I received the following excellent question.
……………………………..
Hello…
I’m a 31 yr old only child whose mother was just diagnosed with squamous cell carcinoma a week ago.
I’m going home for the first time (parents in WI, I’m in IL) since the diagnosis and after reading this blog, I’m not sure what I should say to her. She is a pessimist by nature and already saying she would refuse chemo (the details of her condition and treatment plan are still in the works) so my dad and I need to figure out a way to keep her positive so she can indeed have the support she needs to fight it. I bought some colored paper and was going to list “reasons why you are a fighter” as well as post some motivational sayings/quotes on their bathroom mirrors, but the ones that came to mind now seem like the ones you SHOULDN’T say “you can do this,”,”stay strong,”
Do you have any suggestions on what I could write? Please keep us in your prayers, I am obviously terrified of the road to come.
—– J
……………………………..
My response:
A few quick thoughts for you, J. I am so sorry about your mom’s diagnosis.
My first thought is that you all need time to adjust to the news. The way you react initially is not always the way you feel once you get your feet back under you. She needs a bit of time to not only adjust to the news but also to make this treatment plan. She doesn’t even know yet what she will be potentially recommended for treatment and yet you are expressing desires to coach her on how to feel.
Being supportive does not necessarily mean keeping her spirits “up.” Maybe what she needs right now is support for how she actually feels, not pressure to be acting a certain way. The best way to support her is to listen to her, and not try to tell her how she should feel. Let her adjust. And most importantly, respect whatever she chooses.
We love our families more than anything, but it’s her choice to make how she wants to live her life and how she wants to treat her cancer. It’s enough to deal with these diagnoses without feeling you are carrying the emotional burden of your loved ones on your back too. It will mean that she will know everyone rises and falls on her actions. That’s a huge weight above and beyond the physical and emotional toll she will be going through.
One of the most important things to do is to ask her how she thinks you could help her the most. I have a feeling putting up signs is not it, especially if you say she is a pessimist by nature. Signs around the house won’t change her attitude if a lifetime of experiences haven’t. Loving her, spending time with her, helping her with things that she might have trouble doing… those might be better. The key is to ask, really listen, and then respect what she says. Her needs might change (doesn’t want or need help now but needs it in the future) so you have to ask again during treatment.
If she decides to refuse chemo it will be tough, but it’s her choice. Chemo is very hard and is a quality of life issue too. Depending on what they are recommending and what the ultimate details of prognosis are, it’s important to respect what she opts to do while still encouraging her to see the benefits (as described by her doctor).
Those of us with cancer know everyone wants us to be “strong” and “positive” but it’s what we need to hear the least. It’s not like we haven’t thought of that already; it often just makes us feel like people are telling us how we should act because it makes it better for them if we act that way.
Negative emotions are normal with cancer, especially only one week after diagnosis… how could they not be? Not feeling free to express them may just be one more way she feels burdened by this disease right now.
Clearly you love her and want to help. The fact you are concerned with the best way to support her shows wonderful affection. The best way to do that right now, so soon after diagnosis, is to ask, and then respect what she says… That’s my best advice right now.
She will need time, but ultimately I think that she will be grateful for being allowed to express her emotions both negative and positive. I wish you all the best. Please keep us posted.
May 15th, 2013 §
 I find myself in silence a lot,
I find myself in silence a lot,
Tuning out the noise.
No room for anything but thoughts.
I try to forget for a few minutes,
I stare at a spot on the wall.
I lose myself.
No clue how long it has been.
The clock says it’s been six minutes,
I am glad that they’ve gone by.
But then I realize I have wasted them:
Six minutes of my life.
I want them back,
Feel I should use them for something better,
Something constructive.
I am mad at myself:
That was a waste of time.
I want days of suffering to pass,
But I also know that this is the only time I have.
I take a trip inside my head
I don’t know where I go.
Somewhere else,
Anywhere else,
Far away from here.
If you’d let me, I would run away,
I would go find a way
To keep you safe from this,
Safely far from this.
Some days I long to tell you how I truly feel,
But there’s no room for that in this,
No room for that in this.
It is not a choice.
That I know.
And when I finally do go
It won’t be for lack of want, or heart, or strength.
When I die it will be because that is what cancer is,
This is what cancer does.
And when it comes to being fair,
There is no room for that in this,
No room for that in this.
May 10th, 2013 §
 My mother, Dr. Rita Bonchek, is a psychologist who specializes in grief and loss. A career discussing death and dying, however, was insufficient preparation for hearing the words, “Mom, I have metastatic breast cancer.”
My mother, Dr. Rita Bonchek, is a psychologist who specializes in grief and loss. A career discussing death and dying, however, was insufficient preparation for hearing the words, “Mom, I have metastatic breast cancer.”
Mom and I have reacted very differently to the news of my stage IV cancer. I was online within days writing posts about the steps I was taking. I wrote immediately about how to help children in the days following a diagnosis like mine. As my readers know, I’m very open about this part of my life.
My mother, on the other hand, is much more private. She would never write a blog the way I do. She didn’t want to share this news with people; she wasn’t ready to talk about it. I respect her decision but that approach doesn’t work for me. Sometimes our different ways of thinking lead to disagreements. Despite our differences we always support each other.
I thought it might be helpful for readers to hear what she has to say about reading my posts. Some of us with cancer choose to be very public with our daily lives but our parents are often forgotten in the discussion. I think the timing of Mother’s Day weekend is perfect to share this piece. I love you, Mom (photo at left: 1970).
…………………………………….
 I am Lisa’s proud mother and I have followed her blog from its first day. As her mother, I read her blog from a unique point of view, and I want to share my perspective with you.
I am Lisa’s proud mother and I have followed her blog from its first day. As her mother, I read her blog from a unique point of view, and I want to share my perspective with you.
Those of you who are reading this blog follow Lisa and her incredible writing. It is her understanding of human behavior, her expression of feelings of her heart and thoughts of her mind that make so many people want another blog from her as soon as the one being read is finished.
Yet, as the mother of this outstanding-in-all-aspects daughter, my reading of Lisa’s blogposts is complicated because each piece contains an extra layer of heart-wrenching pain for me. Lisa’s blog is a precious sharing of her everyday life, of medical explanation and analysis of each and every test result, of measured consideration of her hopes, fears, etc. Parents rarely get the opportunity to get “up close and personal” to this extent with a child. As Lisa’s mother, knowing her innermost thoughts is a gift and a curse.
If you (or anyone else but Lisa) were writing about a life journey with a cancer diagnosis, I could handle reading about the physical assaults on your body and the emotional assaults on your psyche because I would be more objective and not involved in your everyday life. I could read your blog, feel empathy and sorrow for the diagnosis, but step away from it. However, I am enmeshed in Lisa’s writing.
Lisa’s father stopped having the blogposts sent directly to his e-mail because he was often caught unaware with heavy emotional subject matter arriving at inappropriate times. He now accesses the blogposts only when he feels emotionally prepared for whatever he may find.
While this would also be a very reasonable decision for me to make, I have the ambivalent feelings of wanting to be close and share every moment of what Lisa thinks and feels at that moment versus retreating from the declarations of how her life is now and her fears for the future for her and the family – her family and my family.
Lisa and I share the personality trait of always wanting to know the truth so we are as well prepared for the worst as we can be. Lisa and I promised each other that we would never withhold any information to protect each other. The honesty Lisa promised me is the honesty she has promised to all of you, her readers.
On one level, her blog reveals to me everything I want to know, but on another level what I unconsciously don’t want to know. This emotional see-saw of wanting to read it but not wanting to read it is a decision that I must make each time a new blog-post appears in my inbox.
Why is this “to know or not to know” decision so difficult for me? When I read Lisa’s writings, I imagine the sub-text that she does not reveal: how she is managing to keep her family’s lives as “normal” (whatever that means) as possible.
Lisa is, as most mothers are, the hub of her family’s life. When Lisa writes in a blog-post that she was very tired and rested for hours, I know that her closed bedroom door makes every family member who sees that closed door go into overdrive with founded or unfounded concern and fear.
Lisa and I share the goals to make the most of each day and to cherish and to love one another. These are life affirmations within our control when so much of life is out of our control. Share our goals as you and I, Lisa’s readers, benefit from Lisa’s greatest gift to us: who she is and how she lives her life, in sickness and in health.
May 2nd, 2013 §
I have my father’s walk,
A slow, deliberate, long-gaited stride.
I have my mother’s smile, her voice, compassion.
I can’t yet see myself in my children,
I wonder if it is always that way.
I remember as a teen the day I actually could match my father stride-for-stride,
My smaller feet dwarfed by his size 13 shoes.
I remember thinking I was a grownup then.
I was wrong, of course.
I had no clue what being an adult was.
I learned.
Yes, I did.
I yearn to go back to those days,
Perhaps I was not carefree but I was taken care of.
Knowing my parents were in charge,
I felt safe, protected.
Now I am a parent in charge,
I must be ready.
My children try to match my steps, still unable to.
I yearn for the day they can.
I hope I will be beside them when they are old enough to mirror my stride.
Not just beside them in spirit.
That’s not enough.
I want more.
When they think they are grownups
I want to be there too.
April 28th, 2013 §
 It is easy to be happy when you are healthy.
It is easy to be happy when you are healthy.
It is harder to know that this may not be true much longer.
People love to casually say,
“Enjoy every moment” or
“We all die some day anyway” or
“Life is fleeting.”
I know this already.
And I know it in a different way.
I don’t need to be told to
fight the good fight to beat it
or the key is to just stay strong
or that it’s mind over matter
or that I should pray for a miracle
or that I will be cured.
That’s nonsense.
Scientifically impossible in my case.
And so, when you say,
“No, that can’t be true.
There must be something that will cure you,
If you want it/pray for it/think it will be so,
You can be healed,”
What you do is force me to assert my knowledge,
Insist upon my diagnosis,
Explain the desperate nature of my disease,
Spend my time defending my sentence.
I know it’s what you wish.
I know you insist because you want it to be the case.
I know you’re grasping at straws,
Wanting to reassure yourself that bad things won’t happen to you,
That bad things don’t happen to good people,
That something awful won’t happen to me.
Trust me, I wish for it too.
But these things do happen.
It has happened to me.
The truth is that wishes don’t count for anything when you’re placing them against cell biology.
I know many healthy people who say the passage of time is bittersweet.
It isn’t a competition but I can tell you that this passage of time is different.
If you could feel it for just a moment you would know.
There is a difference between
Distant,
Hypothetical,
Potential,
Maybe…
and reality.
I have learned that being nervous about test results,
Worrying,
Wondering,
are not the same as the reality.
Reality is having your oncologist walk in the room
and when you say to him, “How are you?”
and he says, “Not good,”
you naïvely think it must be a problem with him,
or his family and
instead he ducks his head,
takes a breath,
looks at you, and says,
“Your test results were not good.
Your tumor markers are up.”
He knows I know what this means.
He waits for a moment and says,
“I think you have a metastasis.”
A few minutes later he says,
“You need to go get a chest x-ray right now.
Go across the street,
I will come over to the hospital and look at it immediately.
Wait for me there.
Then you need to schedule a PET scan as soon as possible.
Have you had any other unusual pain?
A cough perhaps?”
The room spins, the world stops.
My life didn’t end in that moment, but life as I knew it ended for sure.
No turning back.
Reeling, processing, shock.
All you can do is let your jaw drop,
the tears fall,
your body shake,
crumple.
Slowly,
deliberately,
as I looked at him
in a way that I never had in the six years he had been my doctor,
the only words that came to my lips in response
were to repeat over
and
over
and
over
and
over
again:
“Fuck. Fuck. Fuck. Fuck.”
Because that’s the only word that could capture how angry
and scared
and angry
and surprised
and angry
and shocked
and angry
I was.
I never have liked the term “to expire” rather than “to die.”
I started thinking about these words though.
We all have an expiration date.
I’ve never thought of it like that before.
We all have one.
It is as if I’ve grabbed a carton of milk without looking.
I took the one in front I guess,
The one with the rapidly approaching date they put conveniently at the shelf’s edge for people to grab when they’re not paying attention.
Except I did pay attention.
I did.
I was always paying attention.
No one was more vigilant than I.
I want to put this carton back,
I want to say it’s not mine.
I want to scream it.
This must be for someone else.
The date is too soon but I can’t trade it in for a new one.
No givebacks.
The problem is
I don’t know exactly what the date says.
April 21st, 2013 §
 The response to my last post Floating Away was truly overwhelming. Thank you for your responses, comments, and emails last week.
The response to my last post Floating Away was truly overwhelming. Thank you for your responses, comments, and emails last week.
I wrote three pieces while I was in Florida. I was planning to take time off from writing, to focus on the trip, the family time together, the joy. And I did. For most of it. The truth of the matter is that even joy right now is twinged with sadness. The writing I did was on my phone and was explosive and emotional.
That’s just the way it is. What I’m doing is grieving.
It’s been six months since the diagnosis of metastatic cancer. I’ve already run through one chemo regimen, wrung its effectiveness dry, and now have had to move on to something else. It will be at least one month before we know if it is working. There is no way to know if it will, and if it does, for how long. I’ll then be leapfrogging on to the next thing.
The loss of control is hard. It eats at me. I always wanted to believe that if I played by the rules, took the most aggressive route I could with my cancer the first time (more than 6 years ago), that I’d at least be NED for a decade or two. I was told my chance of recurrence was in the single digits. But cancer doesn’t listen to statistics– good or bad. The features of each person’s cancer are different. How aggressive it is, its resistance to certain treatments, its mutations.
I am not a risk-taker by most definitions of risk. I always felt that playing it safe would somehow benefit me.
I have come to believe that what I did actually did matter. I have come to believe it’s that not that it didn’t work. My surgeries, chemo, prophylacic oophorectomy… maybe, just maybe, those things bought me a few years. It’s possible I’d be dead already if I hadn’t done them.
I digress. But I want to reiterate that just because I am writing heavy pieces here, this isn’t the way you will find me if you see me in my daily life. There is joy, happiness, living. Please know that. I’ve always explored the darker emotions, the harder subjects.
Perhaps I feel the written land of the upbeat is for others. My niche is here, in the agony of this disease. There is so much emphasis on “being positive” and all of that; I feel the compulsion to show the flip side, too. I do not want to show the nitty gritty details of what the cancer is doing to me, what my side effects are, what appointments I go to; while important, they are a laundry list. Instead I choose to do what I have been doing all along here: writing my way through the forest of my emotions.
…………………………………
Sometimes as I’m drifting off to sleep I make a sound.
A sudden hmmmmm or a series of loud breaths.
If my child did this as I watched her sleep I’d furrow my brow,
stroke her hair,
pull up the blanket and tuck it under her chin.
But who will do that for me today?
I push them away, it is not time yet.
I do not yet need to be cared for like that.
And yet, I know it will come.
I must fight these demons.
I brave the fear.
I agonize with the decisions.
I push harder than I should.
They are watching.
Always watching for a chink in the armor, a sign of weakness.
No one else can truly understand what each of us with this disease must balance.
Even those of us who have chosen to publicly share our lives with cancer still manage to keep much of it to ourselves.
I do.
I must balance privacy and pain and catharsis.
Many people say they still can’t believe my stage 4 diagnosis.
That denial is a luxury afforded to those who are not compelled to live it.
You must believe it.
We must believe it.
I must believe it.
I have no choice.
It’s my life now.
It’s my death someday.
That noise I make as I fall asleep?
It is the sound of startled agony.
April 18th, 2013 §

I sit on the beach, feel the sand’s angry texture rub my chemo feet in a way I wish it wouldn’t.
I watch my family in the ocean, turquoise and calm and vast.
My husband flips over, face in the water, takes some strokes out to sea. His movement is graceful, effortless, just as it was the when I met him 22 years ago.
He was a sprinter on the college team then, and while he laughs and says it doesn’t feel effortless anymore, nor perhaps fast, it does not matter. In my mind’s eye he is that young man, swimming fast, joking with his team, coming over to the stands to talk to me while chewing on the strap of his racing goggles. I fall in love with him again every time I see him swim.
My three children float, bobbing in the ocean water.
I can feel the distance between us, it feels like a lifetime.
It is my family in the ocean floating away from me.
I see the quartet, I watch as an outsider.
I do this a lot lately. I watch them from afar and think how it will be without me. A new family unit. Behind the big black sunglasses my tears stream down.
Suddenly Tristan is running from the water to me, across the sand. He stands, dripping, face beaming. “I just wanted to tell you I love you, Mama.” I take his picture. I capture the sweetness. I grab him, hug him, feeling the cold ocean water on him, melding it to my hot skin. I murmur to him what a sweet boy he is, that he must never lose that. I send him back to the ocean, away, so I can cry harder.
By the time they return to shore I’ll have myself composed. But my oldest immediately senses something amiss. She mouths to me, “Are you okay?” And pantomimes tears rolling down her cheeks.
Yes, I nod.
I walk to the water’s edge to prove it.
April 12th, 2013 §
I want to just send out a quick clarification about my chemo because I can tell from messages I’m getting that I didn’t explain well what has happened with my discontinuation of Xeloda. This particular chemo is now failing, yes. But that doesn’t mean it didn’t work. This is part of this disease of metastatic breast cancer. In some cases the treatment option never works; that is, your cancer doesn’t respond at all. You get no benefit from day one. You abandon it quickly.
Mine, however, falls into the other camp: it did work for a period of time. It did what it was supposed to, just for not as long as we’d hoped. That is, it did reduce the amount of cancer in my body for a while, it did hold progression at bay.
It’s no longer doing that, my counts are very slowly rising, but that doesn’t mean it “didn’t work.” It just means it didn’t work for as long as I would have liked.
Most people with advanced disease will be leapfrogging around all sorts of agents (chemo, anti-hormonals, etc.) to try to see what works. The cancer mutates and becomes resistant to most treatments that will get used. That’s when it’s time to move on to a different one. I know people that have been on at least ten different agents. That leapfrogging is just the nature of the path many others and I are on. A small percentage find one that works and it continues to work for a long, long time. Research is needed to find out why these particular cancers are more easily tamed. We do not know now why that is the case but researchers are learning more and more about the subtypes.
So while the stability was not as long as we’d liked, in this particular case it doesn’t mean it didn’t work. It did. For six months. But now we’re moving on.
In my case, because my cancer is estrogen-receptor positive, we’re trying anti-hormonal agents. Although I don’t have ovaries to produce estrogen, the fat cells and adrenal glands in my body still produce estrogen. I will be taking two drugs every day now, Aromasin and Afinitor. The plan is in place and I’m already starting taking them, slowly on the Afinitor because it has a side effect of bad mouth sores if started at a full dose. I won’t go into other side effects here because I don’t know yet what my particular response will be.
Thanks for all of the notes of support and concern over the last 48 hours during the PET scan and this new adjustment. As always, I can’t respond to every message but I do appreciate them all.
April 11th, 2013 §
A quick update. I’m sorry to say that my hand-wringing and concern in my last post were met with unfavorable results yesterday. My tumor markers were again slightly higher. In and of itself (an isolated rise) it would be acceptable. But this has been a trend for long enough that it’s evidence my current chemo has failed. Goodbye Xeloda. I’m sorry to see you go. I’d hoped for longer than six months on it for sure.
I’ve got a PET scan early this morning (Thursday). It is being used as much to see how much progression there is as to be used as a baseline before starting the next treatment.
I’m still talking with my oncologists about what the next treatment should be (options include oral anti-hormonals and various IV chemotherapies). Whatever I choose will be ripe with new side effects and demand monitoring. My hands will improve; much as I am happy about that, I am truly sorry to see the Xeloda go. I think you always want to hope that the first thing you throw at this disease will keep you stable for longer than this. But, the Xeloda did good work for six months. But we knew this day would come: on to the next.
I am glad there are still things to try. But of course, for now, I’m sad.
I’m still grieving and angry and all of those emotions. But I’m also learning new skills of compartmentalization and recovery. I move forward, I move on, I live. There is no choice. I change treatments and see what I can get from it. My life has become a puzzle shifting pieces; we move and mix them around until they fit. That fit won’t last, but hopefully it lasts for a while.
Do not be concerned if you don’t see a post for a bit. I’m going into research and decision-making mode. I appreciate all of the support from everyone. I know that if hopes and wishes and hugs could cure my cancer I’d be healthy for sure. I can’t acknowledge all of the messages right now and even the thank you notes for Tristan’s birthday party are sitting half-done. For now this is what I am focusing on and being every bit the mom and wife that I can be at every other moment.
April 9th, 2013 §
 In the still of the evening I hear the frogs waking up to Spring.
In the still of the evening I hear the frogs waking up to Spring.
I hear the creak of the floor as my daughter walks around her room,
Sets things just so,
Murmurs to our dog.
In the still of the evening I hear a car,
A train,
A neighbor calling his own dog home for the night.
In the still of the evening my mind wanders again.
Back.
Always back.
I finished my 13th round of chemo 48 hours ago.
I wonder what is going on inside my body.
I wish I could see.
I wish I knew.
Is it working?
Is this round the one that will show evidence of chemo failure?
Will I move on to a new treatment?
One step closer to the end?
Every time I bang against something,
Every time I feel a twinge,
Every time that fractured bone aches,
I pause.
The pauses add up to moments.
The moments add up to minutes.
I reel them back in like fishing line, I show them who’s boss.
Just listen, I say.
Listen to the frogs. The creaks. The murmuring. The train.
Just listen.
Just hear the quiet,
Hear the house going to sleep for the night.
Feel the love.
Be grateful you can.
April 5th, 2013 §
 For those who wanted to hear my interview on Doctor Radio and weren’t able to listen on Wednesday, here is a link to a downloadable audio file of the one hour show. Thanks to my brother, Mark, for doing this. That show leads directly into today’s discussion.
For those who wanted to hear my interview on Doctor Radio and weren’t able to listen on Wednesday, here is a link to a downloadable audio file of the one hour show. Thanks to my brother, Mark, for doing this. That show leads directly into today’s discussion.
……………………………..
I always get some heat about posting essays about the stupid things people say to those with cancer.
I know people come here expecting to learn. That’s what I’m trying to do: educate. People inevitably vary in their responses to what people say. After all, responses to books, movies, and comedians are all over the place.
Occasionally people will get defensive and say, “Well, I have said one of those ‘stupid’ things and I meant well.” I am going to take an unpopular stance and say that meaning well isn’t always enough.
Maybe the listener is scared. Maybe they’ve had cancer or a family member with it. Maybe they are just uncomfortable talking about illness and death. It’s important to remember: it’s not about you. It’s about the person with the illness. If you are a friend you will need to get over your discomfort or get out of the way. What you don’t want is for the ill person to have to be consoling the listener or trying to minimize the seriousness of what they’re feeling.
Do not turn it back on you, or when you had cancer, or when your child or mother or 2nd grade teacher did. It’s not necessarily the same. Types of cancer are not the same. Even subtypes of cancer are not the same. Now, I’m not saying you should always avoid interjecting something to let the other person know that you’ve had experience with cancer. But the first thing out of your mouth shouldn’t be to connect it to someone else and what their outcome was, good or bad.
Different diseases cannot be compared. Different cases of the same disease cannot necessarily be compared, either. Chiming in with, “Oh, my second cousin’s boyfriend’s dog walker had breast cancer” doesn’t help a person, especially if it’s followed by “She suffered in pain for a long time and died” (yes, this gets said more often than you can imagine). The other end of the spectrum is, “Oh I know someone who had that. They’re fine now.” (Okay, but some people are not fine… should they be jealous? Feel inadequate?) Someone told me in response to learning I had metastatic breast cancer that his wife “had a bit of that last year.”
If you had a coworker who worked the entire time she had treatment, that’s great. We are happy for her, truly. But that bears no relation to how someone else can handle their surgeries, treatments, and side effects. So while you might think it’s supportive (in your mind you’re saying, “See, I’m being supportive and reassuring her that it might not be as bad as she thinks”) what that person may reasonably hear is, “Wow, if you have to take time off work you are weak, or at least not as strong as my coworker was.”
What would be something better to say to a coworker? How about “Please tell me how I can help you during this time. Is there something at work I can do to make it easier for you? I hope you know I would like to help if I can. If you can’t think of anything now, that’s okay. Just let me know if/when you do. I’ll ask again to make sure you’re getting the help you might need.”
Asking “Has this been a good week or bad week for you?” seems like a good bet to ask someone you might not be best friends with. It shows concern and they can be as detailed as they want in their response.
…………………………..
A few weeks ago someone tweeted to me, “As a cancer survivor myself, I know that half the battle is the mindset. Be determined to defeat cancer and you will!” Then followed that one up with “I meant that if we believe we can win against it, we will.”
Comments about someone’s attitude are definite don’ts. Does that mean those who die every day are responsible for their deaths because they are weak-minded? If it were as easy to defeat cancer as mindset, people would not die of it by the thousands every day.
Similarly, comments about appearance while rampant, can strike the wrong chord. I can’t tell you how many times people find out about my stage 4 diagnosis and say, “But you LOOK just fine!” The two are not always correlated, most especially at the time of diagnosis. This is why many people don’t know they have cancer and are completely taken by surprise. When people tell me “You look great!” I know they mean something nice by it. But the rest of that comment, the dark underbelly, is “You don’t look like you’re dying” or in some ways more insidious, “If you look that good you can’t possibly be that sick/it can’t be that serious.”
Don’t say you know exactly how someone feels if you don’t have evidence to back that up. Being a compassionate person and caring friend does not require personal experience that is identical to what the person is going through. Let me say that again, a different way: in my opinion you don’t need to have had cancer to be a caring friend. It might help you to be a good friend if you have had cancer, but it’s no guarantee. People “do” cancer differently. While the experience might have similarities, it doesn’t mean we will necessarily agree on how to deal with it. Part of what I try to do here is level the playing field. I try to bring you information and advice you can use so that you will know more about helping than you did before.
Don’t tell them that their science-based treatments are bunk and what they really need to be doing is just changing their diet, breathing pure oxygen, or relieving their constipation to be cured of cancer. Do not tell someone who is in the middle of treatment that chemotherapy is a waste of time. You may think your suggestions of supplements/vitamins/tea are harmless, however, there are serious interactions that can dull the effectiveness of chemotherapy and other treatments. Not all lotions are good to use during radiation treatment. Not all vitamins are good additions.
………………………….
I like what @travisbhartwell tweeted to me: “Mindset changes the days you have, not the number of days you have.”
The worst thing that can happen is that friends disappear. This is happening to me in spades. It may be that they are afraid they’ll say the “wrong” thing and end up being written about. But I think it also has to do with the fact that death and illness make people uncomfortable. I represent their fears. People who should be in touch with me at least every week or two (because that is how often we saw each other before) have just dropped away.
That said, there are so many people in my life who are so wonderful. Who offer to help, who make it easy to accept it. Who send notes or emails of support months after the initial shock. Who keep asking what they can do. Who pointedly give ways they can help and ask if I could use it.
………………………………..
One thing I think is very important is to always say to someone who is ill or has experienced a death in the family: do not write me a thank you note for this. Do not feel the need to answer this email. Do not feel the need to call me back.
If you live near the person ask them, “Would it be helpful if I texted you before I run errands so that I can pick something up for you?” Texting and email help because talking on the phone is almost always too much of an ordeal and/or inconvenient. I have friends who email me at the beginning of the week to say, “I’ll be at the grocery store, the drugstore, and the post office this week. Can I do anything there for you?” Some will text on the spur of the moment, “Running to Costco. Need anything?” These are invaluable offers.
If you have no knowledge of what information you are being told, admit it. People with serious illnesses do not expect you to know everything about their new diagnosis. They are probably learning a lot of information in a short period of time and may not even know the details of their diagnosis and treatment. They don’t expect you to have the knowledge but you need a way to connect. I recommend when someone tells you about a diagnosis you don’t know much/anything about you say, “I don’t know anything about what that diagnosis means. Would you mind telling me about it, and what it means for you?”
How is it affecting your day-to-day life and what part of that can I help you with?
I’m so sorry to hear that.
What is the worst part of this for you and how can I help make that a bit easier for you?
If your friend is dying or has a relative who is, and they refer to the death or how difficult treatment/daily life is, don’t brush it off, dismiss it, or say, “Oh, you’re not going to die. You’ll be fine. It will all be okay. Things will work out.” Saying this to someone with stage 4 cancer comes across as dismissive of the seriousness of their diagnosis.
If the listener says, “Oh, that’s depressing, let’s not talk about dying,” it can isolate the person who is ill, making them feel they should not be thinking about what is a very real concern or outcome. As Julie Klam points out in her book Friendkeeping, acknowledging someone’s wishes should be paramount. She tells the story of her mother and her mother’s friend Patty who was dying of cancer. Patty wanted to give Julie’s mom a pendant. Rather than gratefully accepting it, Julie’s mom insisted Patty would wear it again, that she would get better. Instead, she died a few days later. Years later when recounting the story with regret, Julie’s mom said, “She knew she was dying. It probably would’ve been comforting to her for me to acknowledge that… I was just afraid that she had some small glimmer of hope. I just didn’t know.” I would bet that if that same scenario happened again, Julie’s mom would act differently.
Later in the chapter Julie recounts being a friend to someone who had to terminate a pregnancy. She asks Julie a question that continues to haunt me: “Will anything ever be good again?” It echoes in my mind now: Will anything ever be good again? Will anything ever be good again?
The truth of the matter is that for some it will. For some people, it won’t.
Check in with your friend intermittently. Give her reminders that she is not forgotten even if she is not out in public. I love getting cards or texts or emails that tell me what my friends are up to. As I write this my friend Kathleen texted me to say she was eating at one of our favorite places. “I miss your company” she said. How can you not love that?
I love written notes. I save my favorites. When I’m having a bad day there is something about pulling out a card, seeing handwriting, reading a message. It’s just more personal than seeing it on a screen. Of course texts and emails are great for frequent check-ins, but for a special message? Real paper can’t be beat.
Other winners to me are notes that remind me of a funny experience a friend and I had, a favorite memory. Many people know I love my garden and flowers. They will send me a pretty card and tell me what they saw at the farmer’s market or in their own garden or what they’re looking forward to about Spring. Sometimes they will tell me about being on vacation and how they thought of me when they saw the water or the tropical plants and they remembered a trip I’d blogged about.
Some send a favorite poem or story or memory. I like those. I don’t like religious quotations or cards that focus on people praying for me or hoping for a miracle. That assumes I am a religious person (I am not and I don’t believe in miracles). I think cards should focus on the person— the connection to that person, your friendship, not what types of religious comfort or explanation the writer endorses.
One Twitter friend, Neil Shurley, wrote me a song titled “We Love You, Lisa,” and then made a video with people holding up signs that say those same words. I still watch it. I always cry. It’s one of my favorite things anyone has ever done for me. This, from what most people would term a stranger. Another friend, Nichole, took photographs that people sent her, combined them with poems and sayings and turned them into a photo book for me. When I’m down it’s another thing I reach for to feel support.
Does the person who is ill have children? If so, you can do what one room mom did for me this year: For school events Lizzie always asked if I felt well enough to join on any party or field trip. She offered rides to school performances. When I could not attend, she (and other moms) took photos and videos and sent them to me… without being asked. My friend Zerlina put together a playdate calendar and a dozen moms signed up in rotation to have Tristan over three times a week for playdates for the past six months. This was especially helpful. Sometimes I’ve been well enough to say we would host the playdate here. But knowing there was fun built in with his friends was a relief to me.
Finally, I always love my mother’s suggestion for one of the best questions you can ask in any situation whether it be posed to a friend, a spouse, a child, a coworker. When someone comes to you with a complaint, a problem, or a rant asking the simple question, “Do you just want me to listen or do you want my advice?” is a wonderful way to be supportive. Sometimes a friend just needs to cry and vent, no advice wanted. By asking you will show sensitivity to the distinction. This is what I mean by not needing to have had the same experience to be a good friend. Listening matters. It’s free, and all you have to do is offer (and follow through).
And if you have a serious illness how do you respond when someone asks you how you are? If you don’t want to answer in detail, one suggestion is to say, “There are good days and bad days. Today is a … day.” This response is also a good one after the death of a loved one. If you are having a good day it allows you to acknowledge they’re not all like that. If you’re having a bad day it expresses that you know they won’t all be like that, either.
……………………………….
I think we all like to hear that we matter, that we make a difference, that we are loved. In the end, you can never go wrong by telling (or writing) someone what they mean to you, what you like about them, and what you enjoy most about being with them. This is the essence of friendship to me. Some days you need a serious chat. Some days you need a friend to be silly with. Some days you need a friend to go shopping and have a gossip session with and try to put cancer in the back seat for a few hours. There are many ways to be supportive.
My dear friend Cathy texts me every morning to wish me a good day and asks, “How can I help you today?” I most certainly don’t expect that every friend should do this. But boy, it means a lot that she does. I rarely need something these days. But I will someday. And when I do, I know she’ll be there for me.
I have so many people in my world who care. I know how fortunate I am. I hope that some of these suggestions will be helpful and I am sure you will find others as readers comment on the post. You don’t need to have many things to say… a few good options will do.
…………………………………….
I hope you all have a good weekend, we are starting to feel Spring here and boy, does it feel good!

 Next week I am meeting with a group of oncology Fellows at Sloan-Kettering to talk about care of the metastatic breast cancer patient. I have many ideas of how I think patients and doctors can better be “partners in care.” I have thoughts about how patients can be better in their interactions but this particular session focuses on the physician side of it.
Next week I am meeting with a group of oncology Fellows at Sloan-Kettering to talk about care of the metastatic breast cancer patient. I have many ideas of how I think patients and doctors can better be “partners in care.” I have thoughts about how patients can be better in their interactions but this particular session focuses on the physician side of it.



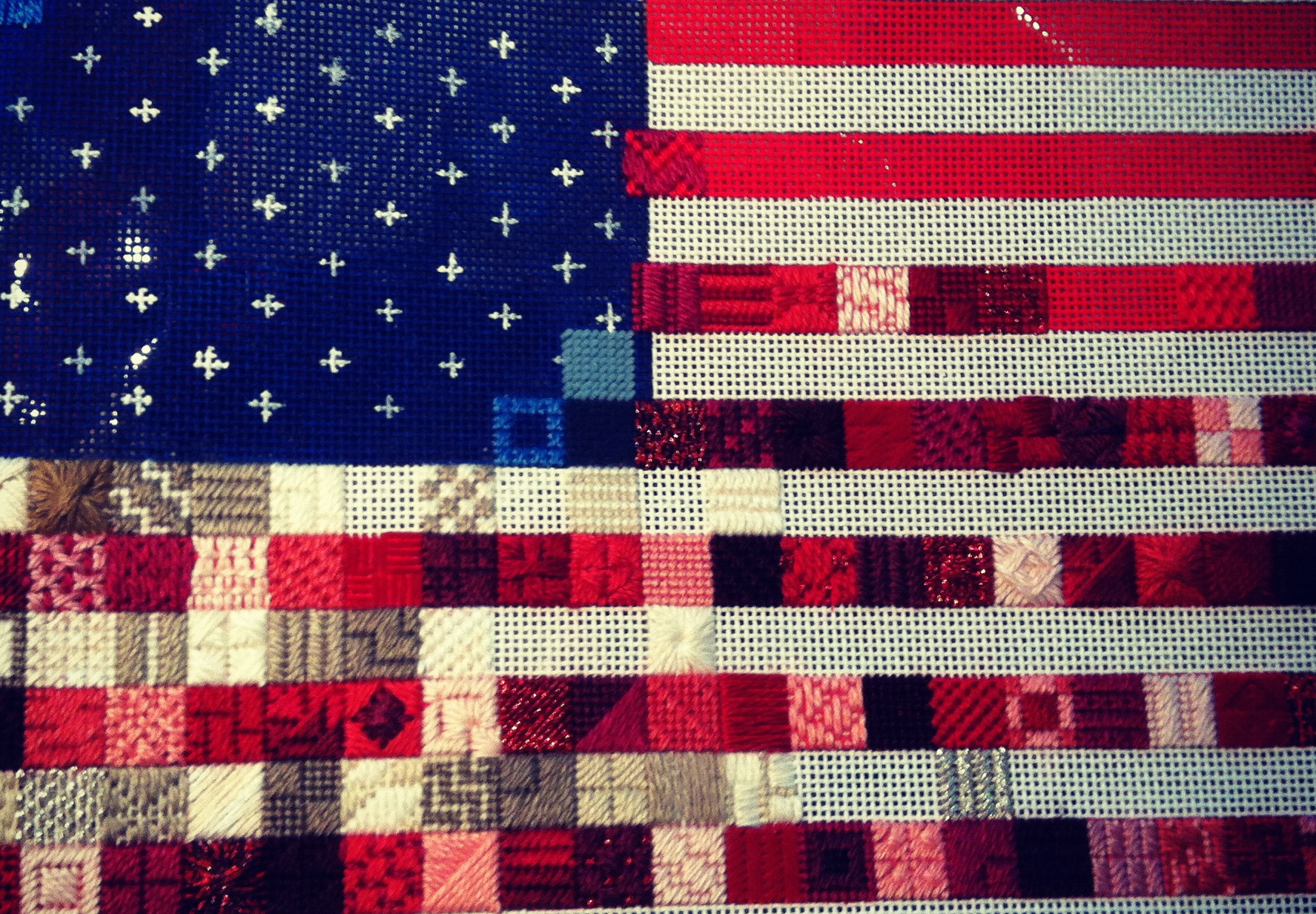





































 Link to Twitter
Link to Twitter